Labour/Delivery– A Normal Physiological process which takes place in the body of a woman at the end of Pregnancy where the fetus is expelled out of the uterus through the Vaginal Canal.
Cesarean Section/Delivery– A procedure conducted in a pregnant woman leading to Birth of a fetus through incisions given over the Abdominal Wall (known as Laparotomy) and over the Uterine Wall (known as Hysterotomy) after the completion of 28 weeks.
Cesarean Delivery dates back to Greek Mythology where the Apollo – “God of Health” had delivered his son Asclepius – “God of Medicine” from Coronis.
The word Cesarean gets its origin from:
- The Legend that Julius Creaser was born in this method.
- A Roman Law – “lex Caesarea”; a procedure performed upon a dying or a dead mother, as an attempt in saving the Child.
- Cedere – a Latin word meaning “to cut”.
Terminology
Terminology related to Cesarean Section (CS):
- Primary CS: Mother operate for the first time for the delivery of the baby.
- Repeat CS: Mother operated for subsequent pregnancies after the first.
- Cesarean Hysterectomy: The procedure of removing the Uterus intra-operatively during the Cesarean Delivery in order to manage a complication.
- Postmortem CS: Cesarean Delivery performed in a mother who has just died or is expected to do so.
- Elective CS: Preplanned, Prearranged procedure during or at the end of pregnancy in the presence of an Obstetrician, Anesthesiologist, Pediatrician and Nursing Services.
- Emergency CS: Procedure done when there is an Acute Obstetric and Fetal Emergency.
Categorized based on the threat to the lives and the time duration between the Decision made and Delivery of the baby.- Cat – 1: Immediate threat to both lives, duration to be within 30 minutes.
- Cat – 2: Maternal and Fetal compromise and not Immediately Threatening, duration to be within 75 minutes.
- Cat – 3: There is no compromise but there is a need of CS as early as possible.
- Lower Segment CS: In this procedure, incision made on the Uterus is in the Lower Segment i.e., extending superiorly from the peritoneal attachment to the level of internal os.
- Upper Segment/Classical CS: Incision is usually made in the Upper Uterine Segment, this incision is taken only if the lower segment is inaccessible and in Postmortem CS.
Reasons for conducting Cesarean Delivery
There is a constant rise in the rate of Cesarean Deliveries in the society. Some of the reasons being:
- Improved facilities including Obstetric Care, Anesthesia, Surgical Equipment, Blood Transfusion, Antiseptic Methods, Post-Operative Care and Nursing Services.
- Average maternal age has been increasing who are nulliparous and at an increased risk of developing Medical and Obstetric Complications during the Pregnancy.
- Easier and Better diagnosis of Fetal Distress, High Risk Pregnancy.
- Rising rates of Induction of Labor which tend to fail.
- Reduction in the rate of Operative Vaginal Procedures.
- Lesser rates for the trial for Vaginal Birth after Cesarean.
- Cesarean Delivery at request.
- Rise in the legal issues in Obstetric Practice.
Indications for Cesarean Delivery can be also be categorized based in the severity of the situation as:
| Absolute – CS is needed for sure. | Relative – Vaginal Delivery can be tried with risk to both. |
|---|---|
| 1. Non Induction of Labor in IUFD 2. Central Placenta Previa 3. Cephalo-Pelvic Disproportion 4. Obstruction to the Passage: Fibroid, Tumor arising from pelvis/uterus/cervix | 1. Repeat Cesarean Section 2. Fetal Distress 3. Abnormal Labor – Dystocia 4. Failure of Labor Induction 5. Mal-presentations 6. Antepartum Hemorrhage 7. Diabetes Mellitus, Congenital Heart Disorders, Hypertension(Eclampsia, Preeclampsia), HIV |
Lower Segment Cesarean Section
(The only type of Surgery performed now)
Pre – Operative Care
- Proper counseling and explanation to be done about the situation, procedure to be executed, complications which may arise pre/intra/post operatively.
- Complete Surgical and Anesthetic fitness to be obtained.
- Patient should be Nil Per Oral from the night before (if Emergency, Ryle’s tube to be placed and contents should be emptied).
- Surgical area to be cleaned and hair to be clipped. (Surgical Area – From Infra-mammary region to the upper half of the thigh.
- Medications – Inj. Ranitidine 150mg / Inj. Pantoprazole 40mg (raise pH), Inj. Metoclopramide 10mg (reduce gastric secretions and increase the tone of LES), Inj. Tetanus Toxoid 0.5ml, Inj. Metronidazole 500mg (or other as per requirements), Tab. Diazepam (reduces anxiety).
- Empty the bladder and rectum.
- Secure an Intravenous cannula and a Foley’s Caterer.
- Administration of Intravenous fluids, preferably crystalloids.
In the Operation Theater
- After the identification of the patient, confirmation of the type of surgery, complete general examination, the patient is hand over to the Anesthetist to administer the Spinal Anesthesia.
- The patient is then placed in the Operation Table in Supine position, the Surgical Area is painted and scrubbed with Bactericidal solution and the patient is draped with the sterile sheets.
- The plane of anesthesia is verified, now the patient is ready for the procedure.
- INCISION: The abdominal wall is first incised, commonly a low Transverse skin incision (modified Pfannenstiel), 3 cm above the symphysis pubis is taken. Rarely, few Surgeons take a Vertical Midline Infraumbilical skin incision.
Taking a Transverse incision has few advantages over the Vertical.
Better wound healing (as along the Langer Lines).
Better Cosmetically.
Post-operative evaluation of the retraction of the uterus is easier.
Less chance of wound dehiscence.
- Dissection is carried out till the level of Rectus Sheath, the Sheath is incised and the muscle is separated in the midline. Peritoneum is incised transversely with the convexity downward
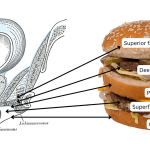
- UTERINE INCISION: There are various types of incisions which can be given over the uterus, the most common used these days is the Low Transverse (A small incision till the membranes is given in the midpoint just below the peritoneal incision and is extended either by splitting the muscles transversely or by using a curved scissors) , others being:
- Classical/Vertical – Upper Segment
- J Incision – Upward Vertical extension the left end of the low transverse
- Inverted T Incision – Upward Vertical extension from the midpoint of the low transverse.
Fig.2 Various Types of Incision given over the Uterus
Low Transverse incision has a few advantages over the others.
Less need of bladder resection.
Less blood loss.
Easy repair.
Less chances of adhesion formation.
Less risk of Scar Rupture during the trial for VBAC.
As
the uterus is visualized, the Vesicouterine serosa is incised and it is
extended transversely which is followed by separation of the urinary
bladder. The uterus is now entered
through various methods as described above. If the placenta is seen through the line of
incision, it first needs to be separated and then the myometrium is
incised. If the placenta had been
incised, fetal hemorrhage is severe and the delivery of the baby and cord clamp
has to be done as soon as possible.
Uterine Incision has to be adequate enough in order to deliver the baby with ease and not to cause fetal or uterine laceration.
- DELIVERY OF THE FETUS: The membranes are ruptured, the surgeons hand is slipped between the uterine wall and the fetal head which is delivered through the incision by flexing the fingers and palm. If the head is stuck in the birth canal, upward pressure through the vagina is applied. As soon as the head is delivered the secretions are cleared off from the nostrils and the mouth to prevent aspiration. The shoulders are delivered through mild traction and mild fundal pressure. And the rest of the body follows.
As soon as the shoulders are delivered, 20 units of Intravenous Oxytocin is administered at the rate of 10 ml/min diluted in a liter of Crystalloid. (To tone the Uterus preventing Hemorrhage)
The Umbilical Cord cut between the two clamps placed and the infant is handed over for resuscitation. The Uterine incision is inspected for any active bleeding an required management is done. A simultaneous Fundal Massage is done to fasten the uterine contraction and placental delivery.
- DELIVERY OF PLACENTA AND MEMBRANES: The separation of placenta is usually spontaneous and is advantageous as there is less risk of Blood Loss and les s chance of retained products of conception in utero which may lead to POSTPARTUM HEMORRHAGE. After the separation the placenta is extracted by cord traction and gentle fundal pressure. The membranes too come out along with the placenta. The uterus is now inspected for any active bleeding points, clots or retained products
- UTERINE and ABDOMINAL CLOSURE: There are two methods which can be followed:
- Exteriorization of the uterus followed by the repair of incision.
- Repair of the uterus within the Abdomen.
There are certain advantages and disadvantages:
When the uterus is lifted out from the abdomen and placed onto the abdomen there is a good visualization of the incision for the repair, muscle tone can be monitored and respective management can be done, any bleeding points may be easily visualized, adnexa are exposed too making tubectomy easier.
The only disadvantage when the uterus is exteriorized in case of regional anesthesia is that it causes discomfort and vomiting.
Following either of the methods the uterine incision is closed in layers, first including the deep layers and the other including the superficial layers and the serosa. The peritoneum is left unsutured. The abdomen is now checked for any fluid or mops which have to be removed. The abdominal wall is closed now in layers including the rectus muscle, rectus sheath, subcutaneous layer followed by the skin suture after wiping the edges of the wound with antiseptic solution. A continuous suture is applied at all the stages. The abdomen is wiped off of the blood stains, vagina is examined for any active bleeding or clots which is managed adequately and a sterile vulval pad is placed. The wound is cleaned with antiseptic solution and an antiseptic dressing is applied.
Upper/Classical Segment Cesarean Section
When exposing the Lower Segment becomes difficult –
- Dense adhesions between the bladder and the lower segment as a result of previous surgeries.
- Leiomyoma, a Uterine Fibroid arising at the lower uterine segment.
- Tumorous growth from the cervix spread to the lower segment.
- Placenta Increta/Percreta, placenta adherent to the previous uterine scar.
- Fetus in transverse lie.
- Evidence of multiple fetuses in utero.
The incision is taken vertically from the lowest possible point extending towards the fundus, until the length is sufficient enough for the baby to deliver without lacerations. Delivery of the baby and placenta is as explained earlier and repair of the incision is done in layers.
Intravenous fluids, blood transfusion needs to be done as and when required based on the intraoperative bleed, antimicrobials needed to be given as soon as the baby is delivered i.e., clamping the cord to reduce the postoperative sepsis.
Post-operative care
- As the mother is shifted to the Post-Operative Room, she needs to be taken care of the anesthetic dose as advised by the anesthetist.
- She needs to be checked for the Blood pressure, Pulse Rate, Urine Output, vaginal bleed, fundal height and the status of the wound and breast.
- Intravenous fluids approximately 2.5-3L within 24 hours and as required based on the intraoperative fluid loss. Blood Transfusion is given if the intraoperative blood loss is greater than 0.5-1L.
- Uterotonics may be given, Oxytocin or Methergine.
- She is allowed to move about, so as to prevent DVT/Pulmonary Embolsim.
- Urinary catheter is retained upto 12 hours to prevent any urinary retention. Also the bowel movements are monitored to manage any postoperative ileus.
- The infant is put onto the chest of the mother (Kangaroo Mother Care) and put for breast feeding.
- The wound is regularly examined so as to check for any signs of wound gaping, seroma or discharge and the antiseptic dressing is changed everyday.
- Oral fluids can be started within 24 hours based in the status of bowel movements, followed by Liquid diet and solid.
- The sutures are removed on day 5-6 of the surgery based on the status of the wound.
- The mother can be discharged on day 3 or 4 unless there are any postpartum complications, provided she is given adequate advice on the restriction of work and the care to be taken at home.
- She has to be advised about breast feeding, frequency and method.
Complications
| Intraoperative | Postoperative |
|---|---|
| Maternal 1. Uterine laceration/Extension of Incision 2. Injury to the Ureter/Urinary Bladder 3. Hemorrhage Fetal 1. Lacerations 2. Aspiration | Maternal 1. Postpartum Hemorrhage 2. Hemorrhagic Shock 3. Endometritis, Cystitis, UTI, Wound Infection, Thrombophlebitis 4. Paralytic Ileus 5. DVT, Pulmonary Embolism 6. Skin Incision complications 7. Incisional Hernia 8. Intestinal Obstruction and Adhesions 9. Scar rupture in subsequent pregnancy Fetal 1. Premature Infant 2. Respiratory Distress Syndrome 3. Asphyxia 4. Sepsis |
Summary
The method of delivering the fetus through an incision over the abdomen after completion of 28 weeks of gestation is known as Cesarean Section.
In the recent years there is a rise in the rate of cesarean section being conducted, most common reasons being past Cesarean Section and choice from the mother.
The most common type of cesarean section practiced is the Lower Segment Cesarean Section.
Upper/Classical CS is done when there is a difficulty in approaching the Lower Segment of the Uterus.
References
- William’s Obstetrics, 23rd edition.
- DC Dutta’s Textbook of Obstetrics, 8th edition.
- Cesarean Section – A Brief History, https://www.nlm.nih.gov/exhibition/cesarean/index.html

Graduated from one of the famous institutions in Telangana, Kamineni Institute of Medical Sciences. He has always been fond of writing articles in Medicine. Since the undergraduate years was interested in making creative Presentations and taking seminars.


it’s really informative
Thank you Sharon… 🙂