Abdominal Trauma
Abdominal trauma can be broadly classified into:
- Blunt
- Penetrating
Both of these have different approach of management.
In case of any trauma, you need to go serially as per ATLS guidelines, i.e., the primary survey followed by the secondary survey.
For quick recap, primary survey includes:
- A = Airway
- B = Breathing
- C = Circulation
- D = Disability
- E = Exposure with environmental control
Note: according to ATLS, C-spine stabilization comes first and foremost; even before airway.
After stabilization of the patient after primary survey we go for secondary survey and management proper of the underlying visceral injuries.
Note: primary survey is comprehended by e-FAST scan which is done bedside within 2-4 minutes.
Blunt Abdominal Trauma (BTA)
Some facts:
- Most common organ injured in BTA: spleen > liver
- Most common organ injured in penetrating trauma: Liver (26%) followed by stomach (17%)
- Most common organ injured in gunshot wound: small intestine
- Most common injured bowel in BTA: jejunum
- Most common injured organ in seat belt injury: mesentery
- Most common injured site in deceleration injury: DJ flexure
- First investigation to be done in abdominal trauma: FAST scan
- Gold standard/best investigation: CECT abdomen
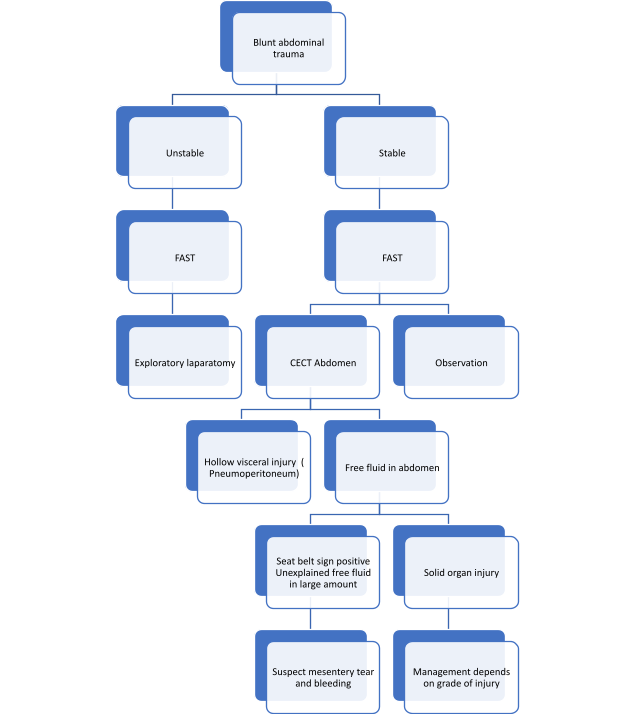
Approach:
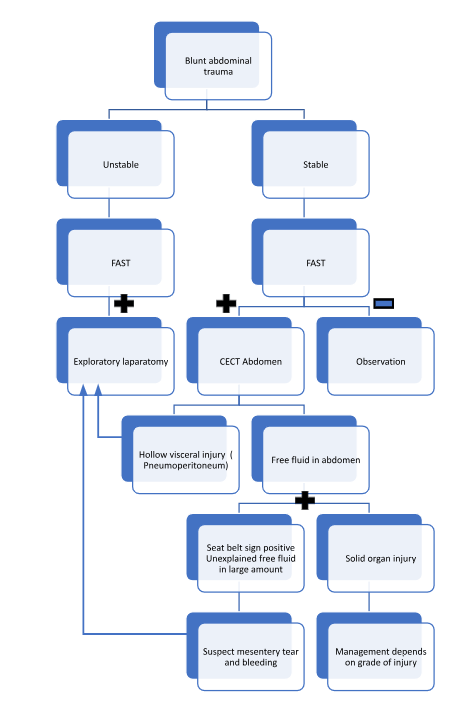
There are no clear-cut criteria to determine stability, but clinically we need to access for:
- Blood pressure
- Heart rate
- Hemoglobin levels
Drop in blood pressure and hemoglobin levels along with tachycardia indicates that the patient is unstable.
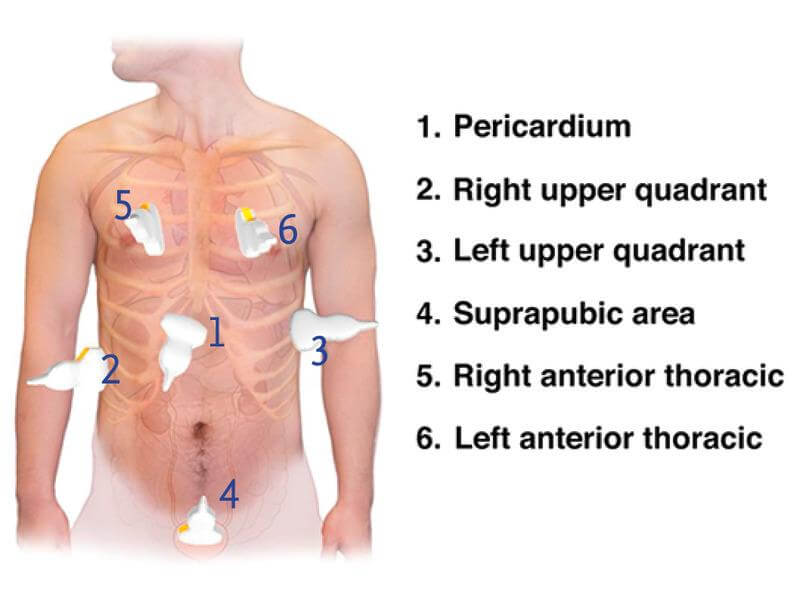
FAST scan:
- Stands for focused assessment with sonography for trauma
- Rapid bedside diagnostic tool to assess patients with thoracoabdominal injuries
- Should be performed within 2-4 minutes
- Should be done in sequence (4Ps):
- Pericardial sac
- Perihepatic
- Peri splenic
- Pelvis
If along with FAST, lungs are also assessed then it is called as e-FAST (extended FAST) which includes right and left thoracic views.
Diagnostic peritoneal lavage (DPL):
- Before the advent of FAST, DPL was widely done
- But nowadays limited to the settings where FAST in not available (in rural settings)
- Performed through vertical infraumbilical incision, Linea alba is incised and catheter is directed towards pelvis
- 1 liter of NS or RL is infused into the peritoneal cavity after catheterization following which the lavage fluid is sent for analysis
DPL is said to be positive when:
- >10 ml of gross blood is aspirated directly from peritoneal cavity
OR
- Any one of following:
- RBCs >1lacs/mm3
- Demonstrable bacteria or bile
- WBCs >500/mm3
- Amylase >174 IU/dL
Sensitivity of DPL: 82-96%
Specificity of DPL: 87-99%
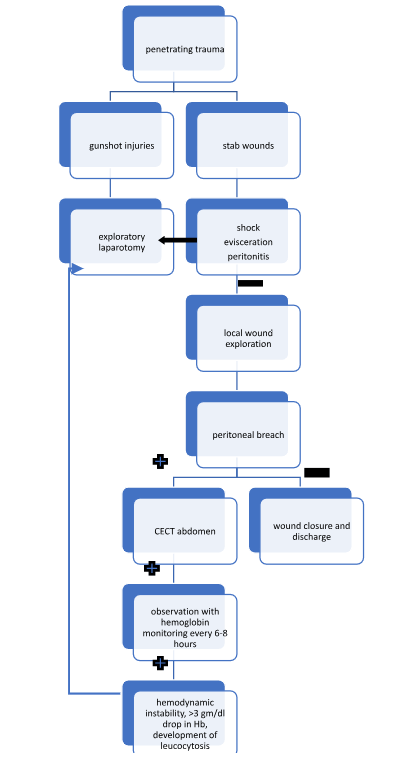
Penetrating abdominal injuries
- Can be divided into high velocity injuries like gunshot where the chances of internal injuries are almost always present which mandates exploratory laparotomy
- Or a low velocity injuries like stab wounds where the need for laparotomy is dictated by hemodynamic stability
Reference: ATLS guidelines 10th edition (2018)

He is an avid reader, guitar player, melodious singer and old songs lover. He has a passion for making medical knowledge accessible and comprehensive.