L-PRF (Leukocyte-platelet rich fibrin) is a second generation platelet reach concentrate where autologous platelets and leukocytes are present in a 3D fibrin mesh which is used as a scaffold by surrounding host cells and which slowly releases growth factors and glycoproteins (≥ 7 days). It is processed without the anticoagulant, which leads to endogenous thrombin formation that activates the contained platelets and also triggers fibrin formation.
L-PRF processing
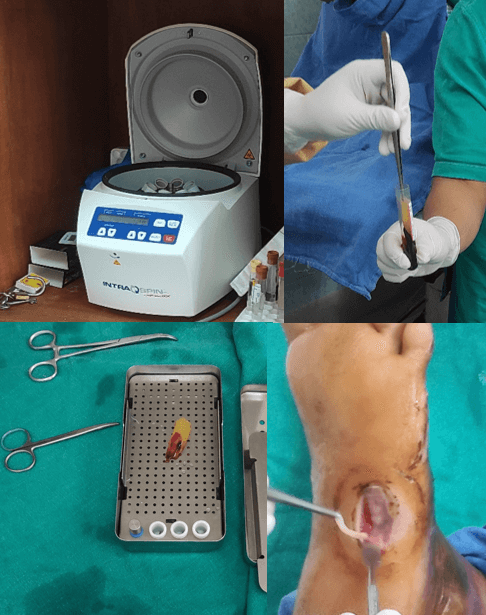
- Blood is collected by venipuncture in 9-10 ml sterile glass of plastic coated tubes without anticoagulants.
- Within 1-2 minutes of drawing blood, the tube is centrifuged at 2700 rpm for 12 minutes (400 relative centrifugal force).
- 3 distinct layers can be seen in the tube:
- Bottom: RBC clot
- Middle: L-PRF
- Upper: PPP (Platelet poor plasma)
- L-PRF can be gently removed from the tube using non-toothed forceps.
- To obtain stronger L-PRF membranes, L-PRF clot is gently compressed in a specially engineered box for 2 minutes.
Composition of L-PRF
- High concentration of platelets (+/- 90% of platelets)
- +/- 65% of leukocytes
- High concentration of growth factors (released over 7-28 days): PDGF, VEGF, TGF
- Representative concentration of fibrin, fibronectin, vitronectin and thrombospondin
Parts of L-PRF
- Head (proximal 1/3rd; closest to red clot)
- Body (central 1/3rd)
- Tail (distal 1/3rd)
With the conventional concept, as the specific gravity dependent fractionation precedes clotting, platelet count is reduced as the distance from the red clot is increased, i.e. the concentration of platelets is highest in the head region.
Applications of L-PRF
- Non-responding skin ulcers: Diabetic foot ulcers, pressure ulcers, acute surgical wounds, and venous leg ulcers.
- Dentistry: Periodontal bony defects, Ridge preservation, Sinus-floor elevation, Implant surgery and to create L-PRF bone blocks.
References:
- Crisci, A.; Benincasa, G.; Crisci, M.; Crisci, F., Leukocyte Platelet Rich Fibrin (L-PRF), a new bio membrane useful in tissue repair: basic science and literature review., Bio. Interface Res. Appl. Chem., 2018, 5, 3635-3643.(PDF) Clinical Trial on Solid 2nd Generation Platelet-Concentrates in the Management of the Chronic Osteomyelitis: A Advanced Regenerative Surgeries. Available from: https://www.researchgate.net/publication/347348923_Clinical_Trial_on_Solid_2nd_Generation_Platelet-Concentrates_in_the_Management_of_the_Chronic_Osteomyelitis_A_Advanced_Regenerative_Surgeries [accessed Apr 10 2021].
- https://www.efp.org/fileadmin/uploads/efp/Documents/Perio_Insight/Perioinsight10.pdf
- Zumstein MA, Berger S, Schober M, Boileau P, Nyffeler RW, Horn M, Dahinden CA. Leukocyte- and platelet-rich fibrin (L-PRF) for long-term delivery of growth factor in rotator cuff repair: review, preliminary results and future directions. Curr Pharm Biotechnol. 2012 Jun;13(7):1196-206. doi: 10.2174/138920112800624337. PMID: 21740372.

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music.