Indications
- Gastric decompression
- Gavage (feeding)
- Gastric lavage (irrigation or dilution of gastric contents)
- Sampling of the gastric contents for analysis
- Sometimes used to instil air into the stomach to detect a gastric perforation on erect CXR
Contraindications
- Basilar skull fractures (Risk of NG reaching brain)
- Facial fractures (risk of cribiform plate disruption and NG reaching brain)
- Obstructed nasal passages (if needed orogastric intubation is considered)
- Caustic ingestion or esophageal strictures (risk of perforation)
- Coagulopathy (Risk of uncontrollable epistaxis)
Characteristics of NG or Ryle’s/Levin tube
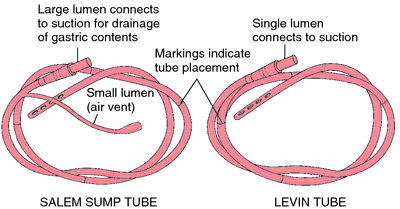
- Length: 125 cm
- Size: Ranges from 6-18 Fr (Adult 14-18 Fr and Child 10-14 Fr)
- Near tip end:
- Numerous side holes
- Radiopaque lead-shots (helps confirm position of NG tube in X-ray and also makes the tip end heavier which helps in insertion of the tube)
- Markings in the body of the tube:
- 1st marking (single line): 40 cm from tip of tube (Tip lies at Gastroesophageal junction)
- 2nd marking (two lines): 50 cm from tip of tube (Tip lies at Body of Stomach)
- 3rd marking (three lines): 60 cm from the tip of tube (Tip lies at the Pylorus of stomach)
- 4th marking (four lines): 70 cm from the tip of tube (Tip lies at the Duodenum)
Instruments needed for NG tube insertion
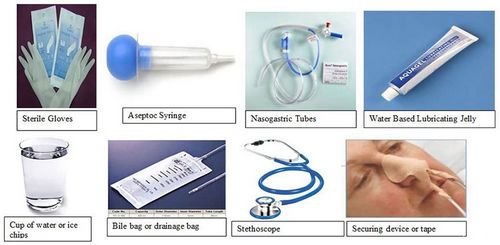
- Clean gloves
- 2% Xylocaine jelly
- NG tube of appropriate size
- Tape for fixing
- Collecting bag
Procedure for NG tube insertion
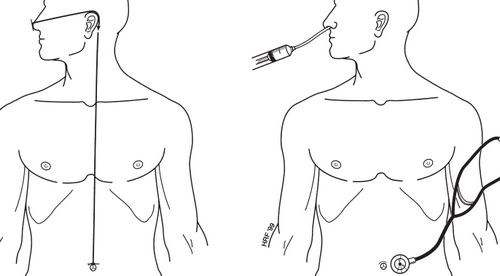
Right: Confirming the correct position of tube
- Explain indication and procedure and take consent
- Estimate the length required for insertion: run the tube from tip of nose to behind the ear and upto the midway between xiphisternum and umbilicus
- Anesthesia:
- Anesthesize nasal passage with local anesthesia
- Lubricate NG tube tip end with xylocaine jelly
- Position: Sit patient upright
- Coil the tube around your hand and begin inserting the tip end through the wider nostril.
- The tip of the tube is directed toward the hypopharynx, not toward the base of the skull. The patient is asked to swallow. Small sips of water through a straw may be helpful
- The tube is advanced as the patient swallows until the estimated length of tubing is inserted.
- Confirming the proper position of the tube:
- Aspirate with syringe – aspiration of gastric contents or bile
- Auscultate on epigastrium – as air is injected into tube with 50 ml syringe (audible gurgling sound)
- Listen to the end of the tube – sound of moving air will indicate the tube is in trachea and not stomach
- Once, the proper placement is confirmed – fix the tube around the nose with adhesives
- Drain the tube into a collecting bag
- Accurate confirmation can later be done before starting gavage feeding:
- pH test: pH < 5.5 with pH paper (not litmus paper)
- X-ray: tip of tube should be below the diaphragm in left side
Aids when you have trouble inserting NG tube
- Commonest sites of resistance at the laryngeal level are the arytenoid cartilages and piriform sinus
- If the tube continually curls up in the pharynx, flex the patient’s neck as much as possible and re-insert, which may change the angle sufficiently to pass an obstruction
- Try placing patient’s head in the lateral position or applying lateral neck pressure (may help prevent impaction of the tube on the arytenoids and in the piriform fossa)
Complications of NG tube
a. During insertion
- malposition (e.g. curling in the mouth or nose, endotracheal and endobronchial placement)
- epistaxsis
- vomiting and aspiration
- placement into the anterior cranial fossa (i.e. base of skull fracture or cranial floor surgery)
- oesophageal variceal hemorrhage (if varices present)
- oesophageal or posterior pharyngeal perforation
b. During use
- sinusitis
- reflux and aspiration
- unplanned dislodgement or migration
- blockage, kinking and knotting
c. During removal
- mucosal adherence and trauma
- failure (e.g. kinking and knotting)
- dislodgement of endotracheal tube (e.g. if NGT is knotted around)


Thanks ☺️ It’s really helpful
Good information….Source of this Article….Books referred