Go through the general principles of orthopedic examination before reading foot and ankle examination.
Look
Look for SEADS GO.
A. Standing
1. From behind:
- Asymmetry of calves
- Swelling of Achilles tendon or posteromedial or posterolateral aspect of ankle
- Tibiocalcaneal angle (usually 5 degrees valgus)
- Visible forefoot (normally 1 and 1/2 toes):
- “too many toes” sign (forefoot abduction in tibialis posterior dysfuction)
- Lumbar spine for signs of dysraphism
2. From anterior:
- Peek-a-boo sign (visualization of medial side of heel in cavovarus)
- Ankle swelling (synovitis, effusion, osteophytes)
- Medial longitudinal arch (normal, planus, cavus)
- Midfoot deformities
- Forefoot deformities:
- Start with hallux and go laterally
- Lateral deviation of hallux: Hallux valgus
- PIP flexion and MTP extension (like boutonniere): Hammer toe
- DIP and PIP flexion and MTP extension (like intrinsic minus): Claw toe
- DIP flexion (like mallet finger): Mallet toe
- Skin and nail changes
- Start with hallux and go laterally
2. Gait
3. Rise on tiptoes (heel raise): screens for functioning gastrosoleus complex
- Heel adopts varus: Functioning tibialis posterior tendon
b. Sitting/Lying: Examine plantar aspect
- Keratoses
- Ulcer
- Orthosis, shoe wear, walking aids
Feel
Feel for TEST CA:
- Follow a systematic approach in a clockwise fashion from medial to anterior to lateral to posterior.
- Harty notch (space medial to tibialis anterior tendon): synovitis, effusion or crepitus can be felt here
- Feel pulses (D.pedis absent in 1/6 patients)
- If a neuropathy suspected, test vibration sense, protective sensation and sense of position
- Anterolateral impingement test:
- Thumb pressure applied over the anterolateral gutter with the foot in plantarflexion will push any hypertrophic synovium into the joint causing pain. If the foot is then moved into dorsiflexion the pain intensifies which is positive for synovial impingement.
- Inferior tibiofibular syndesmosis:
- Tenderness
- Squeeze test: Squeeze at mid-calf level provokes pain
- Dorsiflexion-eversion test: provokes pain
- ATFL
- Sinus tarsi: tenderness in subtalar joint irritation
- Tendon thickening: moves with movement of tendon
- Tendon sheath thickening: doesn’t move with movement of tendon
- Tenderness of anteromedial tuberosity of calcaneus: Plantar fasciitis
- Side-to-side compression of calcaneus: Calcaneal fracture
- Windlass effect/Jack’s test (Passively dorsiflex great toe): Tenses plantar fascia and recreates pain (plantar fasciitis) and restores medial longitudinal arch (flexible flat foot)
- 2nd metatarsal shaft tenderness: Stress fracture
- 2nd MTP joint swelling and tenderness: Freiberg’s disease
- MTP synovitis:
- ‘Daylight’ sign: synovitis pushes toes apart so daylight can be seen between each
- ‘Squeeze’ test: dicomfort
- Tenderness between metatarsal heads (esp. 3rd web space) with burning and paresthesia: Morton’s neuroma
- Mudler’s click: Squeeze and dorsal directed pressure from plantar aspect of webspace produces click
- Pain beneath MTP joint: Sesamoiditis, Degenerative process, AVN, stress fracture
Move
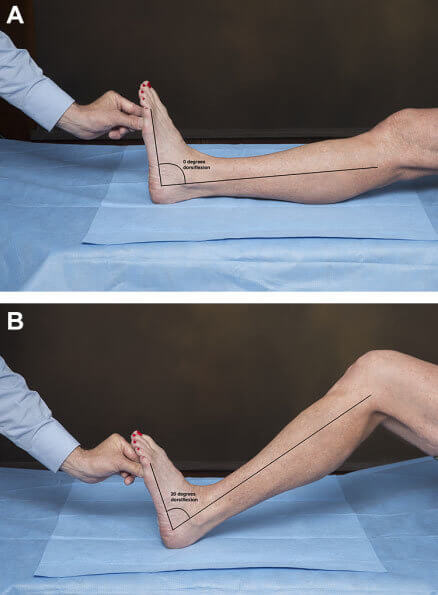
Perform passive then active ROM from ‘neutral’ position of foot.
a. Ankle: Passive movement must be assessed with forefoot in supination and inversion of heel (to exclude dorsiflexion at chopart’s joint and midtarsal joint and to lock subtalar joint).
With legs hanging from couch (knee flexion) and knee extension:
- Dorsiflexion: 0-15 degrees
- Plantarflexion: 0-40 degrees
Silverskiold test for decreased ankle dorsiflexion:
- Dorsiflexion in knee flexion> in knee extension: isolated gastrocnemius contracture
- Dorsiflexion in knee flexion = in knee extension: both gastrocnemius and soleus contracture
b. Subtalar: Lock ankle by ensuring plantigrade position when heel is moved –
- Inversion: 30 degrees
- Eversion: 15 degrees
c. Midtarsal: Fix calcaneum (heel) with 1 hand and move forefoot:
- Abduction: 5 degrees
- Adduction: 5 degrees
d. Mobility of 1st TMT joint: Fix tarsals with 1 hand and move 1st metatarsal up and down (may be contributing factor in hallux valgus and may need Lapidus fusion)
e. Toes:
- Dorsiflexion of great toe at MTP: 70 degrees
- Plantar flexion of great toe at MTP: 10 degrees
Special tests
1. Coleman block test:
- Indication: Cavovarus foot to differentiate if it is fore-foot driven or hind-foot driven and if it is fixed or flexible
- Fore-foot driven: Neuromuscular causes (CMT, spinal dysraphism)
- Tripod effect (1st MT head, calcaneus, 3rd MT head): Plantar flexed 1st MT (due to sparing of peroneus longus) pulls hindfoot into varus
- Hindfoot driven: Trauma (varus malunion of talus fractures)
- Fore-foot driven: Neuromuscular causes (CMT, spinal dysraphism)
- 2.5 cm (1 inch) block or book is placed under foot such that 1st ray is unsupported
- Hindfoot varus corrects: Fore-foot driven and the hindfoot is flexible
- Hindfoot varus doesn’t correct: Hind-foot driven or hindfoot is rigid
2. Single leg tip toe test (heel raise):
- Near wall so that patient can lean to support
- Standing on tip-toe: normally heel will go into varus and medial longitudinal arch is elevated (windlass effect)
- If tibialis posterior tendon dysfunction:
- Double heel raise: affected foot remains in valgus
- Single heel raise: cannot perform on affected side
3. Muscles around ankle:
- Tibialis posterior: Resisted inversion at plantarflexion
- Tibialis anterior: Resisted dorsiflexion with some inversion
- Peroneus longus: Resisted plantarflexion and eversion
- Peroneus brevis: Resisted eversion in neutral position