1. Sepsis presenting with Diabetic ketoacidosis like feature in Preterm neonate
A thriving preterm neonate had new onset sepsis with off color skin and poor feed tolerance. A workup for sepsis was sent and antibiotics were upgraded to 2nd line agents. Inotrope was added for tachycardia with poor perfusion. By evening, there was polyuria with >8ml/kg/hr of urine. We checked our list for any drugs and checked RBS – it was high, so GIR was decreased. By night, baby developed acidotic breathing with severe metabolic acidosis with high blood sugar and urine sugar + ketone +. Fluid corrections were started and was managed with Infusion of Insulin. Over next 12-24 hours the blood sugar came down to < 150mg/dl. Insulin was stopped and there were no further episodes of hyperglycemia. HbA1c was normal. Baby did well with normal Head scans.
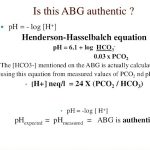
The most interesting thing was the Blood sugar in this baby reached upto 1500mg/dl with ABG ph- 6.9 and HCO3 upto 4meQ/L.
2. Infective endocarditis in a preterm newborn
A baby who was ventilated for poor respiratory effort at birth was extubated on day 4 but started developing features of Congestive cardiac failure in late 2nd week. Baby had murmur since Day 2 but we noticed changing nature of murmur and deteriorating cardiac functions. Baby was started on diuretics and also needed Digitalization. Baby remained CPAP dependent. ECHO was requested. Echo located vegetation in RVOT. The baby also had repeated anemia. In background of all these, we started the therapy for IE. Baby remained 50 days in hospital and was discharged with good feeding and weight gain. Adequate control of failure and will follow up soon for repeat ECHO.
3. IUGR baby with recurrent hypoglycemia : Congenital adrenal hyperplasia
A male baby was transferred in for lethargy and low blood sugar. Despite all management and adequate control of sepsis, it was difficult to wean the baby from IV drip. In background of hyponatremia, hypoglycemia and dark stained genitalia, 21 OHP level was sent which came high and significant. As sample was sent at time of illness, a repeat sample was sent that confirmed CAH. Baby was started on steroid and weaned off IV. Baby was sent for Endocrine consult for optimal care.
4. Down Syndrome with Upper GI obstruction
In view of bilious vomiting and double bubble appearance on Xray, a preliminary diagnosis of Duodenal atresia was made. Baby was operated and on laparotomy has Annular pancreas. A duodenoduodenostomy was done.

5. Three cases of severe Meconium aspiration with PPHN : Sildenafil magic
For a resource limited condition like ours where NO is a dream, so is HFV, we administered sildenafil. The baby’s Oxygenation index decreased over next 12-24 hours and were quickly weaned off ventilators in 2-3 days. A renewed lives from lost hope. One thing that clinicians have to beware is, it can cause refractory hypotension and should be used with caution. It should be avoided in cases with hypotension.
6. Recurrent SVT in neonate
It was the first time, we had to use Adenosine in neonate. This was case in India during my course.
7. Corpus callosum Agenesis, ambigious genitalia with refractory seizure
Baby had atypical genitalia. USG revealed Lissencephaly with corpus callosum agenesis. Baby developed refractory seizure and was difficult to control with 3 antiepileptics so was kept on midazolam infusion. Baby ultimately expired. This was also case seen in India.
Diagnosis was X-linked lissencephaly with absent corpus callosum and ambiguous genitalia (XLAG)
8. Congenital Diaphragmatic hernia to CCHD to Holoprosencephaly
A newborn was referred in suspicion of CDH. Baby was cyanosed at birth. On examination, the findings were inconsistent with diagnosis. Chest Xray ordered showed good delineation of diaphragm on both sides. A suspicion of Congenital heart disease was made. Examination showed a huge posterior and anterior frontanels with diasthesis of suture. Baby had mid-facial hypoplasia with depressed nasal bridge. USG cranium was ordered as such that revealed, Holoprosencephaly. MRI was planned.
9. 1st TEF repair
EA/TEF was first time repaired in our teaching hospital with success. Baby was taken on academic bed and all procedures was done free of charge. The baby has undergone esophageal dilatation few times and is thriving well. With no other organ involvement, we expect the baby will have near normal outcome. This was an endeavor of Pediatric surgery team Neonatology team, Pediatrics team and Ped Gastroenterologist. None of the less the anesthesia team.

These are some of interesting mention-able cases in last one year. Hoping to see more challenging cases in coming future.

MD Pediatrics and Fellowship Neonatology, he chooses to stay anonymous. He often writes his views online as well as share few important topics for medical students, doctors and specially parents. He does research in pediatrics.