Synonyms:
- Of Myringotomy: Tympanotomy (Opening the middle ear cavity), Tympanostomy (Instillation of a ventillation tube), Myringocentesis
- Of Ventilation Tube (VT): Grommet, Pressure Equalization Tube, Ear tubes, Tympanostomy tubes
Definition of Myringotomy
Myringotomy is the incision on the tympanic membrane to remove accumulated fluid or to provide aeration in case of malfunctioning eustachian tube. Ventilation tubes (VT) are small prosthetic tubes open at both the ends and are inserted into the incisions during myringotomy.
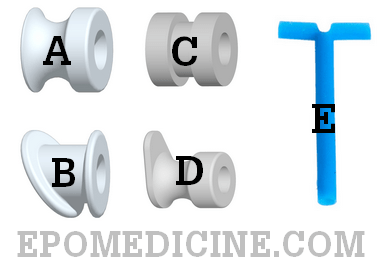
B: Armstrong’s grommet
C: Donaldson’s grommet
D: Shah’s grommet
E: T-tube
Types of Ventilation Tubes (VT)
1) Grommets (dumbbell shaped): Short stay tubes that gets extruded within 6 months
- Shephard’s grommet
- Armstrong’s grommet
- Donaldson’s grommet
- Shah’s grommet
2) T-tube (‘T’ shaped): For long term purposes that stays atleast 1-2 years
Indications for myringotomy
a. Acute Suppurative Otitis Media (ASOM) with:
- Bulging tympanic membrane about to perforate
- Small or too highly seated perforations
- AOM with complications like mastoiditis, facial paralysis, etc.
- AOM with failed medical treatment for 48 hours
- AOM in infants
b. Chronic secretory otitis media/Otitis media with effusion (OME)/Glue ear
c. Aero-otitis media
d. Atelectatic ear
e. As a step in cortical mastoidectomy
Indications for Ventilation Tube insertion
- Chronic OME: unresponsive to antibiotics and has persisted for > 3 months when bilateral or > 6 months when unilateral or earlier if hearing loss >25 dB
- Recurrent AOM i.e. ≥3 episodes in 6 months or ≥4 episodes in 1 year
- Recurrent episodes of OME not meeting the criteria of chronic OME but the cumulative duration is considered to be excessive
- Suspected or present suppurative complications
- Eustachian tube dysfunction with or without OME
- Otitis barotrauma
Preoperative assessment
- Pneumatic otoscopy to confirm the diagnosis
- Pure tone audiometry within preceding 3 months, or age appropriate hearing test, as well as tympanometry
- Examination of nasopharyngeal and neck to rule out pathology that may block eustachian tube and metastasis
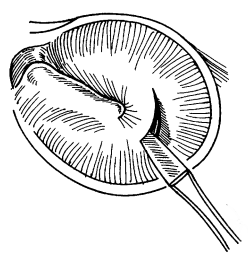
Procedure of Myringotomy
1. Anesthesia:
- Local anesthesia (adults): 1 cc of 1% lidocaine with epinephrine 1:100,000 injection OR Topical phenol
- General anesthesia: for infants, children or in cases of acutely inflamed tympanic membrane
2. Position: Supine with the head turned towards the side of affected ear
3. Sterilization of ear: Clean wax/debris
4. Incision: Through ear speculum, incision is made on tympanic membrane using myringotome:
- ASOM: circumferential incision in Postero-inferior quadrant
- OME: radial incision in Postero-inferior or Anterio-inferior quadrant
Note: Incision in postero-superior quadrant is contraindicated due to risk of injury to the ossicles and chorda tympani and incision is preferred in antero-superior quadrant is optimal for prolonged tube insertion as epithelial migration responsible for tube extrusion is slowest in this quadrant.
Beer can principle: In OME with thick fluid, 2 incisions are made – in Anteroinferior and Anterosuperior quadrant
5. Suction: of the discharge
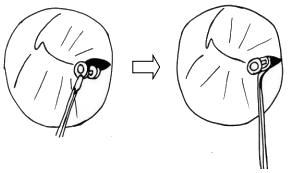
6. Insert ventilation tube: using alligator forceps if indicated
7. Ear drops: may be administered after insertion of ventilation tube and may be necessary to be administered for few days
Contraindications: Intratympanic glomus tumor (risk of profuse bleeding)
Complications of Myringotomy
a) Myringotomy:
- Injury to incudostapedial joint or stapes
- Injury to jugular bulb in cases of high jugular bulb or dehiscent floor of middle ear
- Middle ear infection
- Injury to external canal skin
b) Ventilation tube:
- At surgery: Displacement
- Immediate Post-operative: Plugging, infection
- Delayed Post-operative: Segmental atrophy of tympanic membrane, Tympanosclerosis
- After removal: Residual perforation
Post-operative care:
- Use medicated ear drops
- Prevent entry of water for atleast 72 hours
Displacement of ventilation tube into middle ear:
- During surgery: Instillation of saline through the myringotomy incision will float the tube which can be suctioned
- Post-operative: If the perforation has healed, the tube can be left inside as it is biocompatible and normally does not cause foreign body reaction