Following are the important features of fetal circulation:
1. Placenta plays the role of lungs; lungs are not functional:
- Like pulmonary veins, left umbilical vein carries highly oxygenated blood from placenta to heart.
- Like pulmonary artery, right and left umbilical arteries braing deoxygenated blood to placenta.
2. Mixing potentially occurs at 4 sites:
- Left umbilical vein (Oxygen saturation ~80%) – Portal vein (Much bypassed by ductus venosus to Inferior Venacava)
- Left umbilical vein – Inferior venacava – Portal vein (Oxygen saturation of IVC blood is ~65%)
- Superior venacava – Right atrium (Much bypassed by Foramen ovale)
- Pulmonary veins – Left atrium (Much bypassed by Foramen ovale and ductus arteriosus)
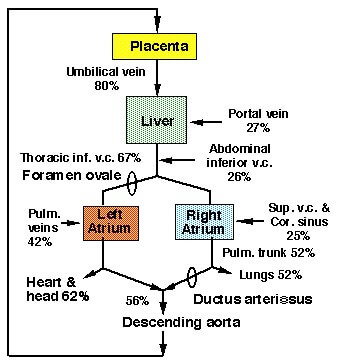
Oxygen saturation of blood in various vessels:
- Umbilical vein: 80%
- Abdominal IVC and portal vein: 28%
- Thoracic IVC: 67%
- Superior venacava: 25%
- Pulmonary veins: 42%
- Pulmonary trunk: 52%
- Umbilical arteries: 56%
Overview of Fetal Circulation:
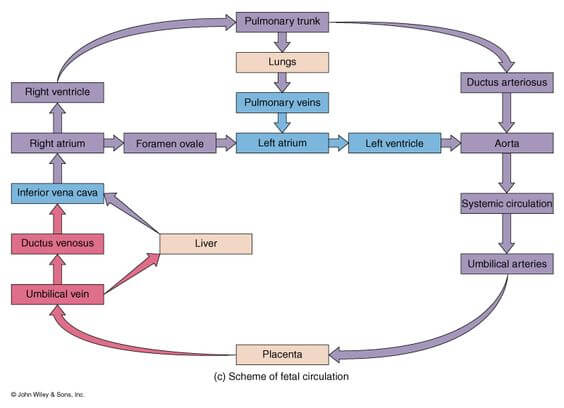
- Blood is oxygenated in the placenta.
- Highly oxygenated and nutrient-enriched blood returns to the fetus from the placenta via the left umbilical vein.
- Some blood enters liver sinusoids; most of the blood bypasses the sinusoids by passing through the ductus venosus and enters the inferior vena cava (IVC)
- From the IVC, blood enters the right atrium, where most of the blood bypasses the right ventricle through the foramen ovale to enter the left atrium.
- From the left atrium, blood enters the left ventricle and is delivered to fetal tissues via the aorta.
- Poorly oxygenated and nutrient-poor fetal blood is sent back to the placenta via right and left umbilical arteries.
- Some blood in the right atrium enters the right ventricle; blood in the right ventricle enters the pulmonary trunk, but most of the blood bypasses the lungs through the ductus arteriosus.
Fetal Combined Cardiac Output (CCO) Distribution:
The 3 shunts of Fetal Circulation:
| Location | Shunt | Between | Function | Closure | Remnant |
| Pre-cardiac (Venous) | Ductus Venosus | Left umbilical vein (Remember: Left is left and right regresses) and Inferior Venacava (IVC) | Bypasses portal circulation
Has sphincter mechanism:
| Functional: With umbilical cord clamping, venous return in the IVC decreases and reduction of flow through ductus venosus allows passive collapse.
Anatomical: Proliferation of the obliterating tissue in specially structured border strips by 15th to 20th days. | Ligamentum venosum |
| Cardiac | Foramen Ovale | Left atrium and Right atrium | Blood from IVC directly flows to Left atrium due to the valves in IVC i.e. Right atrium only acts as a conducting pathway
| Functional: With the 1st breath – septum primum is pressed agains septum secundum
Anatomical: Fusion of 2 apposed septa in about 1 year | Fossa ovale |
| Post-cardiac (Arterial) | Ductus Arteriosus | Pulmonary artery and Aorta | Blood enters Right ventricle through the Right atrium from:
Pulmonary circuit is bypassed due to high resistance in pulmonary vessels – blood flows from pulmonary artery to aorta via ductus arteriosus. | Functional: Within 48 hrs if birth by muscular contraction
Anatomical: By intimal proliferation; takes 1-3 months. | Ligamentum arteriosus |
Fate of Umbilical Vessels:
1. Umbilical arteries:
Functional closure: Immediately after birth due to thermal and mechanical stimuli and increased oxygen tension leading to constriction.
Anatomical closure: By fibrosis; takes 2-3 months
Remnants:
- Distal part: Medial umbilical ligaments
- Proximal part: Superior vesical arteries
2. Umbilical vein:
Obliterates shortly after birth like ductus venosus.
Remnant: Ligamentum teres hepatis

Rally easy
Thnx for making it easy and tidy
This is one of the most sorted flow chart …