Re-dislocation rate after primary open reduction: 0-14% [1]
- higher in medial approach
Causes and timing of failure of primary surgery:
| Postoperative period | Causes |
| Immediate | Approach related, Technical errors |
| Delayed (After 4-6 weeks) | Inadequate capsulorrhaphy, Inadequate immobilization |
| Late | Abnormal remodeling of acetabulum and femur |
Across multiple studies, inadequate soft tissue release – specifically the psoas tendon, the tight transverse acetabular ligament (TAL), and the anteromedial capsule was the most common cause [1,2].
Timing for revision surgery:
There is no universally defined timeline for when to perform revision surgery after a failed open reduction in DDH. Most authors advocate for a waiting period of several months. At least 6 months of interval is recommended between the first and second operations [1,3]:
- to achieve the greatest range of motion
- to allow for maturation of the scar tissue (to become more stretchable)
- to avoid extensive bleeding from the immature highly vascular tissue
Surgical approach for revision surgery:
The systematic review found that in 90% of cases, surgeons chose the anterolateral (Smith-Petersen) approach [1]. The core components of a successful revision include:
- Meticulous Soft Tissue Release: All obstructing structures must be addressed.
- Concentric Reduction & Capsulorrhaphy: After ensuring a stable reduction, a robust capsular repair is performed, excising redundant capsular tissue.
- Pelvic Osteotomy: Pelvic osteotomy is frequently required for acetabular insufficiency [2]:
- Salter osteotomy (to increase anterolateral coverage)
- Dega osteotomy (to increase anteroposterior coverage)
- Khairy Modified Lance Acetabuloplasty (KMLA): for bipartite acetabulum
- Zigzag osteotomy combined with fibular allograft (ZOFA): effective alternative [3]
- Femoral Osteotomy (Varus +/- Derotation +/- Shortening): Often required if not done during primary surgery or a revision required if undertaken during primary surgery
- Adjunctive Stabilization: When stability remain suspicious after all procedures, K-wire fixation can be used to maintain concentric reduction for 6 weeks [2].
Postoperatively, a double hip spica cast in 20° abduction and 40° flexion is maintained for 6-12 weeks, followed by an abduction brace [2].
Outcomes and complications of revision surgery in DDH [1]:
- Clinical outcome: 29.5% achieve excellent results and 5.5% achieve poor results with Ponseti or MacKay clinical scoring
- Radiological outcome: Only 11% achieve normal hip (Severin grade I) and most of them (50%) achieve Severin grade II hips
- Avascular necrosis (AVN): Most common complication (5-67%)
- Femoral shortening osteotomy can lower the risk [2]
- Re-dislocation after revision surgery: 6-13%
- Limb length discrepancy: 9-47%
- Sciatic nerve injury: 1 case reported [2]
Modified Severin classification:
| Severin grade | Criteria |
| I | Congruent hip with no deformity (A – CE angle >19 degrees; B – CE angle 15-19 degrees) |
| II | Congruent reduction but deformity at femoral head, neck or acetabulum |
| III | Dysplasia but no subluxation (CE angle <19 degrees) |
| IV | Subluxation |
| V | Articulation with false acetabulum |
| VI | Redislocation |
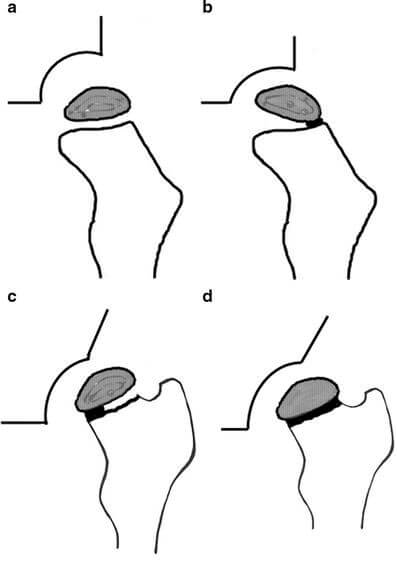
b. Grade II – Lateral physeal damage
c. Grade III – Central physeal damage
d. Grade IV – Total damage to the head and physis
References:
- Merckaert, S., & Zambelli, P.-Y. (2023). Treatment perspective after failed open reduction of congenital hip dislocation. A systematic review. Frontiers in Pediatrics, 11, 1146332.
- Elzohairy, M. M., Elhefnawy, M. M., & Khairy, H. M. (2020). Revision of failed open reduction of developmental dysplasia of the hip. Clinics in Orthopedic Surgery, 12(4), 542-548. (Reference from systematic review)
- Hung, N. (2016). Revision of Outcomes and Complications Following Open Reduction, and Zigzag Osteotomy Combined with Fibular Allograft for Developmental Dysplasia of the Hip in Children. Open Journal of Orthopedics, 6, 184-200.

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.