Synonyms: Bernese osteotomy, Ganz osteotomy
Introduced by: Dr. Reinhold Ganz in 1984 in Bern, Switzerland
Definition:
- Triplanar peri-acetabular osteotomy
- For adults & adolescents with dysplastic hips
- That require correction of congruency & containment to the femoral head
Outcome of 1st Ganz cohort in 30 years followup:
| Authors | Follow-up | Journal | No. of patients (hips) | Survivorship |
| K.A Sienbrock et.al. | 10 years | CORR 1999 | 63 (75) | 80-90% |
| Simon D et.al. | 20 years | CORR 2008 | 58 (68) | 60% |
| T. Lerch et.al | 30 years | CORR 2017 | 63 (75) | 30% |
Advantages of Periacetabular Osteotomy (PAO):
- Posterior column preserved
- Fragment perfusion maintained
- Large acetabular fragment
- Close-to-joint osteotomy:
- Allows medialization
- True pelvis dimensions maintained
- Good improvement in CE angle (avg. 31 degrees correction)
Indications:
- Age: 10-35 years
- Osteoarthritis: Tonnis grade 0-1; grade 2 (selected cases only)
- PAO more cost-effective if no complications
No signs of OA + No previous surgeries + Age <30 years = Success rate almost 100% at 15-22 years followup
For Tonnis Grade 3 OA: Total hip arthroplasty is more cost-effective
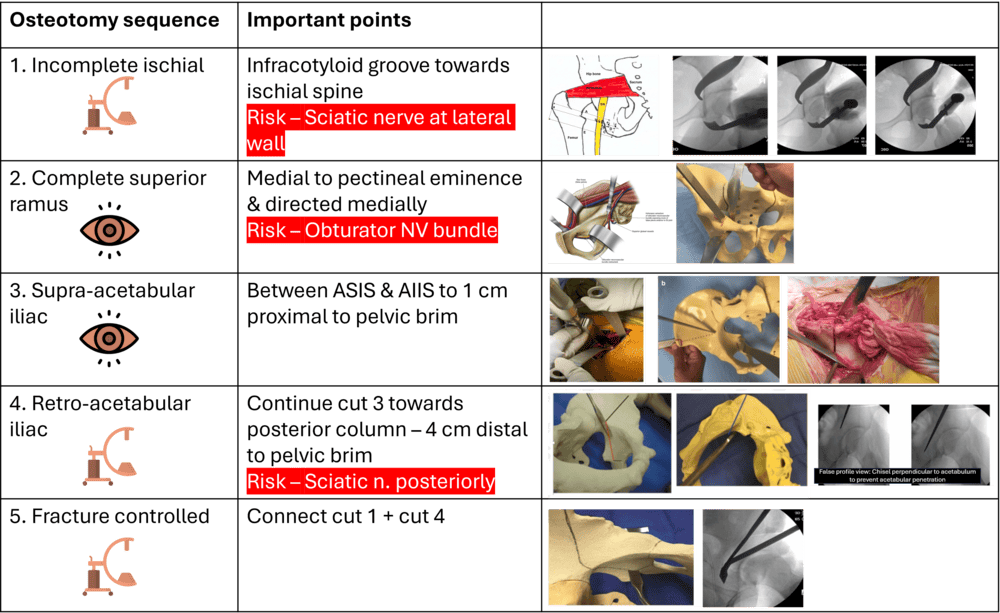
| Osteotomy sequence | Important points |
| 1. Incomplete ischial | Infracotyloid groove towards ischial spine Risk – Sciatic nerve at lateral wall |
| 2. Complete superior ramus | Medial to pectineal eminence & directed medially Risk – Obturator NV bundle |
| 3. Supra-acetabular iliac | Between ASIS & AIIS to 1 cm proximal to pelvic brim |
| 4. Retro-acetabular iliac | Continue cut 3 towards posterior column – 4 cm distal to pelvic brim Risk – Sciatic n. posteriorly |
| 5. Fracture controlled | Connect cut 1 + cut 4 |
Fragment mobilization, reorientation and fixation
Aim:
- Adequate acetabular roof angle (0-10 degrees)
- No cross-over sign
- Femoral head sitting neutrally
Fragment movement: Usually flexed & adducted for “classic dysplasia” but must be individualized
Intraoperative pearls and pitfalls
- Preserve posterior column continuity for stability.
- Use fluoroscopy extensively for blind cuts (ischial, posterior) to avoid joint penetration or incomplete mobilization.
- Common risks: Intra-articular extension, neurovascular injuries
References:
- Bernese periacetabular osteotomy, K A Siebenrock, E Scholl, M Lottenbach, R Ganz. Clin OrthopRelatRes 1999
- Mean 20-year Follow-up of Bernese Periacetabular Osteotomy. Simon D. Steppacher, Mortiz Tannast, Reinhold Ganz, K.A Siebenrock. Clin OrthopRelatRes (2008)
- One-third of Hips After Pericetabular Osteotomy Survive 30 Years With Good Clinical Results, No Progression of Arthritis, or Conversion to THA. Till Dominic Lerch, Simon Damian Steppacher, Emanuel Francis, MortizTannast, K.A Siebenrock. Clin OrthopRelatRes (2017)
- Rodrigues VB et al. Periacetabular hip osteotomy for residual dysplasia. Rev Bras Ortop. 2018;53:332–6.

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.

The 30-year follow-up data showing a 30% survivorship is a sobering reminder of the long-term challenges in treating hip dysplasia, especially compared to the near 100% success rate for patients under 30 without prior arthritis. It is particularly valuable to see how the PAO’s ability to maintain true pelvic dimensions allows for such significant CE angle corrections while preserving blood supply, offering a compelling alternative to total hip arthroplasty for the right candidates.