Before closure of triradiate cartilage (14 in boys and 12 in girls), pelvic bones are weaker than pelvic ligaments leading to more pubic rami and iliac wing fractures. After closure, they are more likely to sustain fractures of acetabulum, diastasis of pubic symphysis and SI joint separation.
Hence, a pediatric pelvic fracture is an indicator of high energy trauma, and the focus must be shifted for possible coexisting systemic complications, extremity fractures and head trauma. Unlike adult conunterpart, pediatric pelvic ring injuries rarely require surgical management.
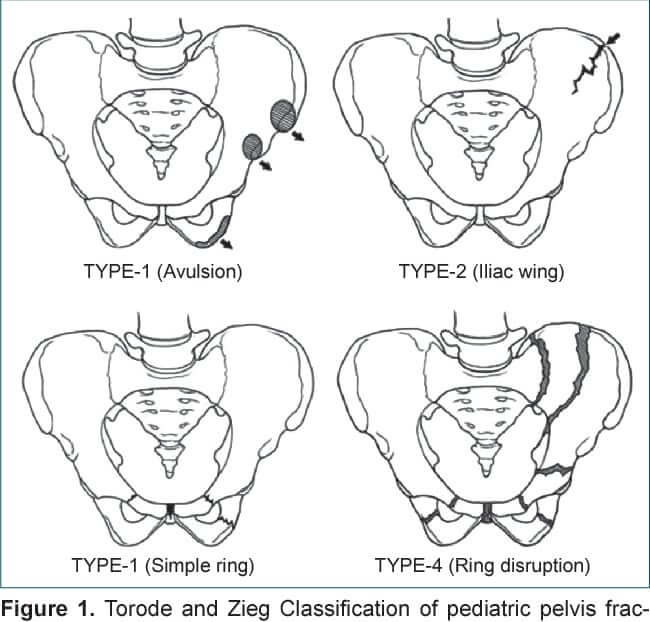
Torode and Zieg Classification
- Type I: Avulsion fractures
- Type II: Iliac wing/apophysis fractures
- Type III (most common; more than 50%): Simple ring fractures without clinical instability
- Pubic rami fractures
- Pubic symphysis disruption
- Type IV: Ring disruption fractures with clinical instability
- Bilateral pubic rami fractures (straddle fracture)
- Type III with posterior pelvic ring fracture or sacroiliac joint disruption
- Type III with acetabular fracture
Shore and Torode modification of Torode and Zieg Classification
Type I and II are same as in the original fracture classification.
Type III is further divided into:
- Type III-A: Stable anterior ring fractures
- Type III-B: Stable anterior and posterior ring disruptions
- Increased need for transfusion, increase length of stay, more frequent admission to ICU and more associated injuries
Type IV: Unstable pelvic ring disruptions with gross clinical instability or >2 mm displacement of both anterior and posterior pelvic ring fractures
Ogden Classification
1. Avulsion injuries
2. Stable pelvic ring fracture patterns
- Infolding of iliac wing
- Iliac crest apophysis avulsion
- Isolated ischiopubic ramus fractures
3. Unstable pelvic fractures
- Unstable rami fractures accompanied with displacement of ischiopubic fragment from symphysis
- Anterior symphyseal diastasis or pubic rami fractures and posterior sacroiliac joint disruption
Other classifications
For mature pelvis, we use pelvic ring injury classification as for adults:
- AO/OTA
- Comprehensive Tile classification
- Young-Burgess classification
References and further reading:
- The Pediatric and Adolescent Hip – Essentials and Evidence (2019)
- https://ota.org/sites/files/2021-06/Pediatric4%20Fractures%20of%20the%20Pelvis%20%26%20Acetabulum.pdf

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.