Today in the OR, I observed a retrograde percutaneous screw fixation of a left posterior column acetabular fracture in a 63-year-old male. While I wasn’t scrubbed in, it offered a fantastic opportunity to understand the precision and fluoroscopic guidance required for this minimally invasive approach. It is often said that, “Percutaneous fixation is a surgery performed by the fluoro tech, where the surgeon assists him/her”.
Let’s break down the surgical steps, the C-arm views, and the anatomic principles behind the technique.
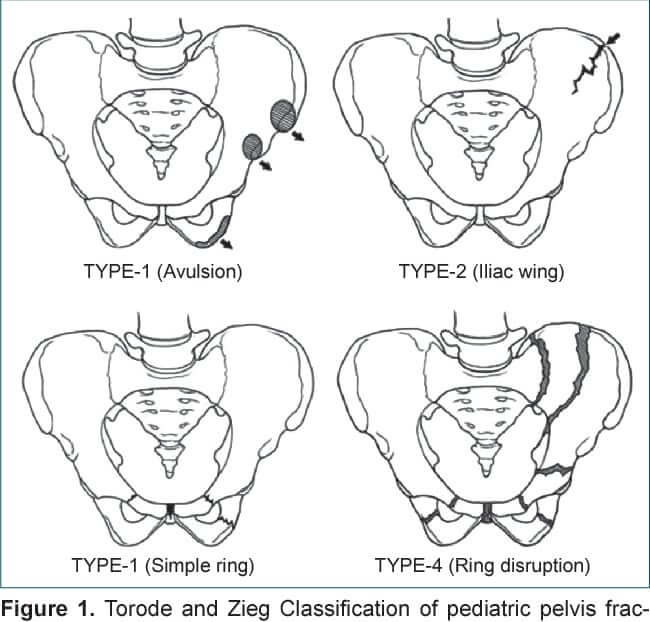
Indications:
- Posterior column fracture of acetabulum, typically seen in elderly patients or after high-energy trauma.
- Displacement was minimal to moderate, allowing for percutaneous fixation without formal open reduction.
Retrograde technique: useful in low posterior column acetabular fractures
Technique:
1. With the hip flexed approximately 45 to 60 degrees (one person must hold the leg in this position), a 2 cm incision is made over the ischial tuberosity. The patient must also be bumped enough to allow access to the ischial tuberosity.
2. The starting point is found on the ischial tuberosity and meticulous nick and spread technique is vital. Staying medial on the tuberosity protects the sciatic nerve (this is lateral).
3. The drill guide is placed onto the ischial tuberosity.
4. A long guidewire is inserted and its placement confirmed utilizing fluoroscopy.
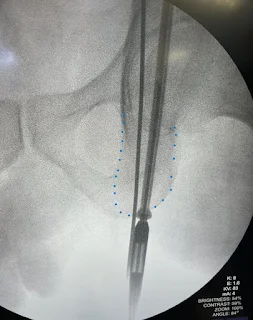
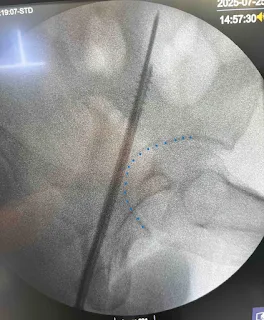
- Obturator outlet view – confirms that you are staying within the posterior column and staying medial on it
- Rotate C-arm 45 degrees towards affected side and 20-30 degrees towards feet
- Iliac oblique view – confirms that the screw is extra-articular
- Rotate C-arm 45 degrees away from affected side
5. Insert 6.5 mm cannulate cancellous screw (CCS) over the inserted guidewire after drilling through using the cannulated drill.
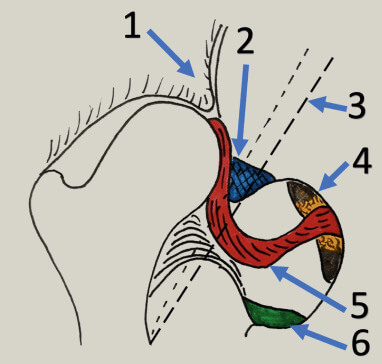
Avoid breaching through 3 things:
1. Hip joint
2. Sciatic notch
3. Cortical walls
During this procedure, I had another question in my mind – how far is the sciatic nerve from iscial tuberosity?
In a study by Murasko MJ et.al., the distance from the lateral border of the ischial tuberosity to the medial border of the sciatic nerve was greater in all subjects in the hip-flexed position versus the extended position. The mean distance was 17 mm (range, 14-27 mm) in the hip-extended position and 39 mm (range, 26-56 mm) in the hip-flexed position ( P < 0.001).
Reference: Murasko MJ, Nourie B, Cooley MR, Chisena EN. The Anatomic Position of the Sciatic Nerve During Percutaneous Retrograde Posterior Column Fixation Is Determined by Hip Position. J Orthop Trauma. 2024 Jan 1;38(1):e1-e3. doi: 10.1097/BOT.0000000000002713. PMID: 37817321.

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.