Dr. Sulabh Kumar Shrestha1, Dr. Rajendra Aryal2, Dr. Nitesh Raj Pandey2, Dr. Bibek Banskota2
1AKBEF Fellow, 2Unit-1 (Hip, Pelvi-acetabulum & Arthroplasty), B&B Hospital
Poster presentation at Orthocon 2026
Introduction
Progressive hip subluxation is a common orthopedic problem in children with cerebral palsy (CP), with strong correlation to Gross Motor Function Classification System (GMFCS).1
| GMFCS I | GMFCS V | |
| Hip dislocation | 0% | 90% |
| Reimer’s migration (MP) | 0.2%/year | 9.5%/year |
Hip dislocation in CP is caused by 5 factors:
- Muscle imbalance (spasticity of hip adductors & flexors & weakness of hip abductors & extensors)
- Increased femoral anteversion
- Increased femoral neck shaft angle (NSA)
- Acetabular dysplasia
- Pelvic obliquity
Painful hips in CP are common and proportional to the extent of hip displacement and GMFCS level.2
Management requires early identification, risk stratification, & morphology-based surgical correction.
Objectives
To demonstrate:
- Principles of management of neuromuscular hip dysplasia in CP
- Long-term radiographic outcomes following surgical correction
Case Description
A 9-year-old boy with:
- Spastic Cerebral Palsy
- GMFCS Level IV
- Dislocated left hip
- Associated acetabular dysplasia
The child had progressive displacement with functional limitations in sitting and mobility.
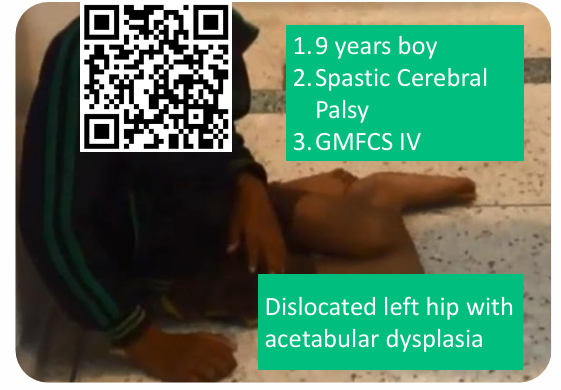
functional video demonstrating floor mobility.
Why Reduce the Hip?
Reduction and reconstruction are necessary to: 3
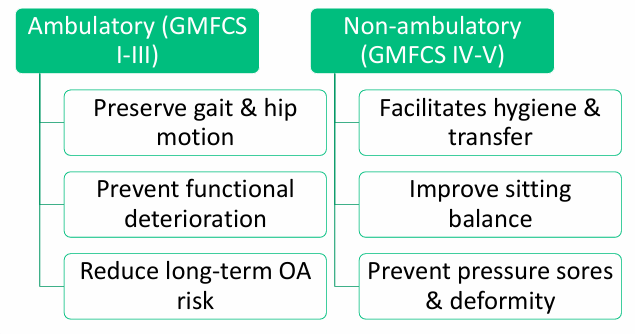
Hip dysplasia in CP is progressive and GMFCS-dependent. Untreated subluxation may lead to painful fixed dislocation.
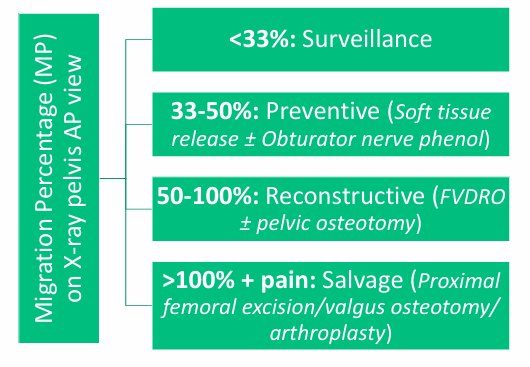
How we do it?
Management is based on Reimer’s MP (RMP): 4
What we did?
A single-stage multilevel interventions were done.
| Primary pathology | Targeted surgeries |
| 1. Muscular imbalance | Adductor tenotomy + Anterior release |
| 2. Coxa valga | Varus osteotomy + Shortening |
| 3. Increased femoral anteversion | Derotation osteotomy |
| 4. Acetabular dysplasia | Dega acetabuloplasty |
| 5. Spastic posterior chain | Hamstring release + Vulpius procedure |
Results (Radiographic outcomes)
A. Serial X-rays
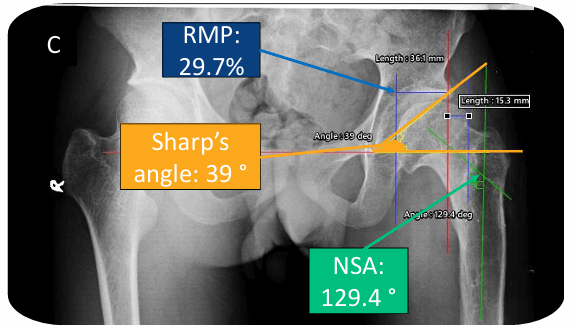
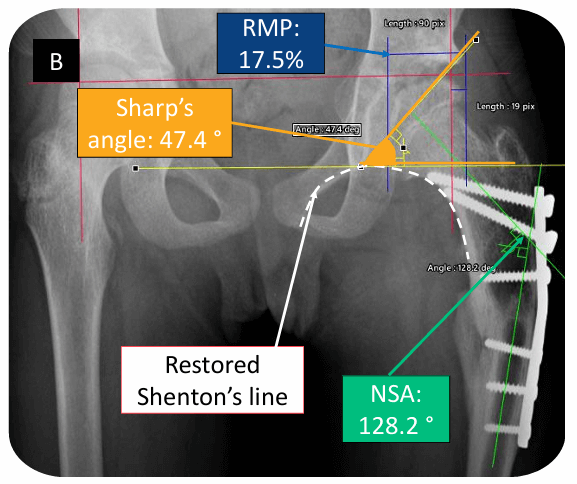
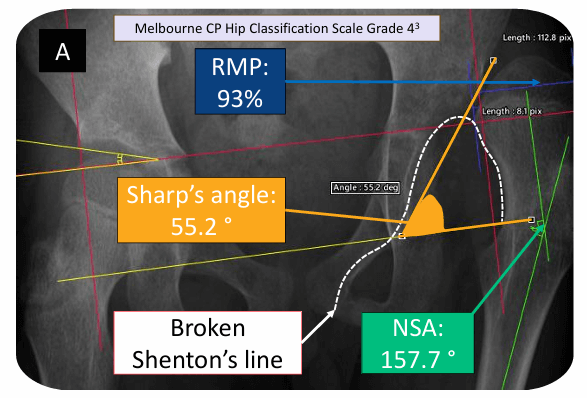
Fig. 2: Radiographic measurements (RMP: Reimer’s Migration Percentage; NSA: Neck Shaft Angle)
A – Preoperative; B – Early postoperative; C – At 11 years followup
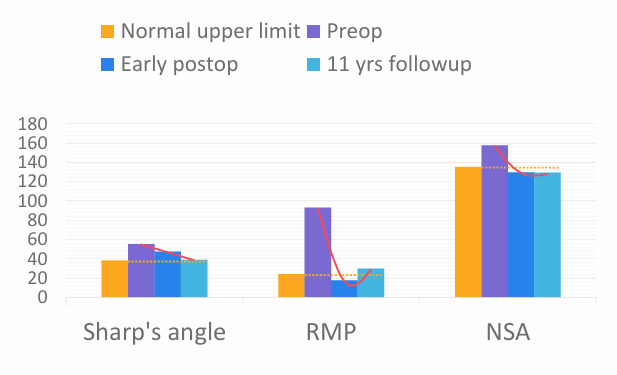
B. Quantitative comparisons over time
Discussion
- Radiographic parameters showed early and sustained correction to maturity.
- Hip dysplasia in CP is progressive and GMFCS dependent.
- Treatment must address femoral and acetabular pathology together.
- RMP guides surveillance and intervention timing.
Conclusion
- A structured decision-making approach is essential in neuromuscular hip dysplasia.
- Early, comprehensive reconstruction can maintain hip stability and long-term function.

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.