Hemoglobin Switching mnemonics 1st to appear: Embryonic hemoglobin (Gower and Portland) Switch from fetal hemoglobin to adult hemoglobin: “Gamma goes, Beta becomes, Alpha always” Fetal hemoglobin: α2γ2 Adult hemoglobin: α2β2 ζ chain α chain ε chain HbE Gower 1 HbE Gower 2 γ chain HbE Portland I HbF β chain HbE Portland II…
Author: Epomedicine
PGMEE, MRCS, USMLE, MBBS, MD/MS
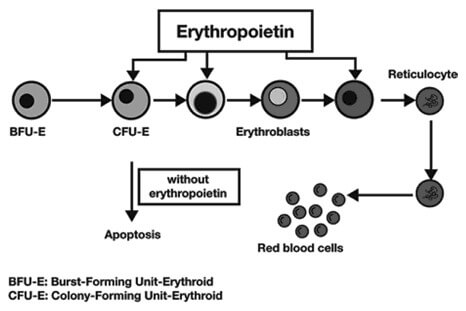
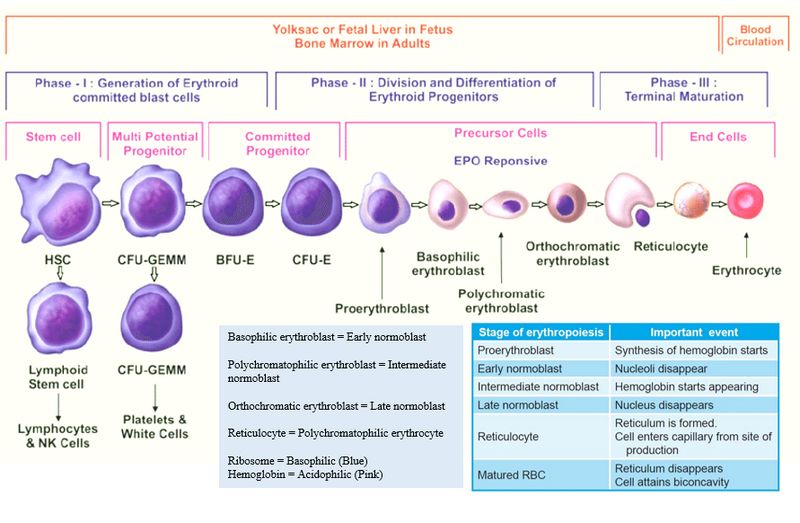
Erythropoietin (EPO) Physiology
Structure of erythropoietin (EPO) Glycoprotein hormone 165 amino acids Molecular mass – 30 kDa Site of production/synthesis of erythropoietin (EPO) Kidneys (75-90%): Peritubular interstitial cells Liver (15%; chief source in fetus and neonates): Centrilobular hepatocytes After birth, erythropoietin is not detectable until 8-12 weeks after birth leading to physiological anaemia…
Clinical Skills and Approaches
Medical Significance of Bedbugs
Two species of bedbugs bite people: the common bedbug (Cimex lenticularis) and the tropical bedbug (Cimex hemipterous). These bugs are called udus (उडुस) in Nepali and khatmal (खटमल) in Hindi language. The adult bedbug is the approximate size, shape, and color of an apple seed. They are more commonly associated…
Blog

How to talk to your kids about drugs ?
Many communities around the country are faced with the reality that an alarming number of young people are trying tobacco, alcohol and other dangerous drugs. Many others are using them regularly. The numbers can be startling. The National Institute on Drug Abuse reports that by the 8th grade, 30% of…
Blog

An Unforgettable Night During Gyne/Obs Rotations
That night, I reported to the L&D floor just like any other night that week. It started off normally with the usual sign out with the residents and then checking the OR board to see if there were any cases to cover. I noticed a D&C up for grabs, so…
Blog
Dr. Govinda KC
Who is Dr. Govinda KC (गोविन्द केसी) ? Better known as: GKC Names given by media: Fasting doctor, Nepal’s Edhi, Occupation: Senior Orthopedic surgeron at TUTH (Tribhuvan University Teaching Hospital), Kathmandu, Nepal Reason for Limelight: Series of Fast-unto-deaths to put pressure on the government to stop the rampant commercialisation of medical…
Blog

Top 10 Medical Colleges of Nepal (Ranking)
While there are about 19 medical colleges currently running in Nepal and few more waiting for approval, there is no official body to rank them scientifically based on academic or other criterion. The Webometrics Ranking of World Universities is produced by Cybermetrics Lab (CCHS), a unit of the Spanish National Research…
PGMEE, MRCS, USMLE, MBBS, MD/MS
Aplastic Anemia : Review notes
Definition Failure of bone marrow to produce peripheral blood cells and its progenitors Etiology The following illustration gives a brief idea about the etiological factors of aplastic anemia Now going into each etiological factor: – Autoimmune diseases: – Either they affect all the lineages (autoimmune aplastic anemia) or a single…