Priming
Administration of a small sub-paralyzing dose of non-depolarizing muscular blocking agent (usually 10% of the intubating dose) is given 2-4 minutes before administering a 2nd large dose for tracheal intubation to accelerate the onset of non-depolarizing NM blockade by 30-60 seconds.
Mechanism and Concept of Priming
2 theories have been proposed:
1. Post-synaptic theory:
- Priming dose: saturates about critical mass of post-synaptic nicotinic receptors (about 75%) but remains subclinical in neuromuscular effects.
- Intubating dose: needs to block only remaining (~25%) of the receptors – hence, the onset of action is more rapid.
2. Pre-synaptic theory:
- Priming dose: blocks presynaptic nicotinic receptors, reducing the mobilization and release of acetylcholine.
- Intubating dose: produces effect more rapidly due to decreased neuromuscular transmission by acetylcholine.
Use
High-dose rocuronium (0.9 mg/kg or 1.2 mg/kg) is often the first choice to secure an airway when succinylcholine cannot be used. Priming is an alternative to high dose rocuronium in such cases.
Disadvantages
- Diplopia (due to sensitivity of extraocular muscles) or mild dyspnea can be distressing to patient.
- Risk of aspiration: Some patients may show signs of muscle weakness following the priming dose.
- Residual muscle relaxation: On emergence, upto 75% receptors may remain blocked.
Precurarization
Succinylcholine remains the drug of choice in conditions where rapid paralysis and airway control are priorities. Precurarization is the administration of a small dose (10% of ED95) of a non-depolarizing neuromuscular blocking agent (NDMBA) a few (3.5-4) minutes before Succinylcholine (SCH) to minimize these complications of SCH use like fasciculations, rise in intragastric pressure and rise in ICP. The required dose of SCH following pre-curarization dose is higher by about 50-100%.
Mechanism and Concept of Precurarization
Mechanism of fasciculations and rise in intragastric pressure by SCH: Fasciculations are caused by antidromically conducted axonal depolarizations initiated by the agonist action of SCH on pre-junctional nicotinic receptors at the neuromuscular junction, leading to the simultaneous contraction of all muscle fibres of individual motor units. Rise in intragastric pressure have been shown to be due to fasciculations. Raised ICP has been attributed to raised PaCO2 due to fasciculations.
Pre-curarization or Defasciculating dose: Small dose of NDMBA blocks pre-junctional nicotinic receptors earlier NDMBA with preference for pre-junctional nicotinic receptors (e.g., d-tubocurarine) may be the best choice to block this effect of SCH, without antagonizing the post-junctional (paralyzing) action of SCH, or causing weakness themselves. Rocuronium is an acceptable alternative.
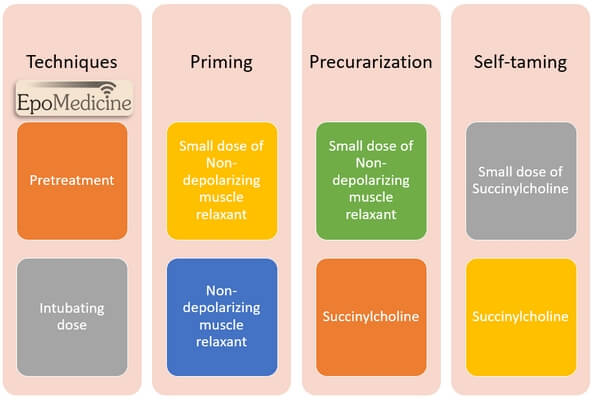
Self taming
Self taming is a technique whereby a small amount (0.1 mg/kg) of succinylcholine (SCH) preceding the administration of full intubating dose (1 mg/kg in adults) during rapid sequence induction (RSI) to decrease the incidence and extent of fasciculations.
Concept and Mechanism of Self taming
The taming effect of the pretreatment dose may be attributed to the induction of neuromuscular desensitisation or accommodation. The depolarisation achieved by the subsequent dose of succinylcholine may therefore be enough to produce neuromuscular block without reaching the threshold necessary for electrical excitation of the nerve terminals and the muscle membrane.
References
1. Clinical Anesthesia 6th edition – edited by Paul G. Barash
2. Trauma Anesthesia 2nd edition – edited by Charles E. Smith
3. Precurarization – John E. Cannon MD FRCPC; CAN ,l ANAESTH 1994 / 41:3 / pp 177-83
4. Anesthetic Pharmacology: Basic Principles and Clinical Practice 2nd edition edited by Alex S. Evers
5. Pharmacology for Nurse Anesthesiology – Richard G. Ouellette, Joseph A. Joyce