Dura mater (pachymenix) is the outer meningeal layer consisting of:
Outer endosteal/periosteal layer: Firmly attached to the periosteum of the calvarium
Inner meningeal layer: Gives rise to dural reflections and continues into foramen magnum as spinal dura
Dural Reflections
These are the infoldings formed by the inner meningeal layer reflecting away from the fixed periosteral dural layer.
Two vertical reflections – Separate the right and left hemisphere
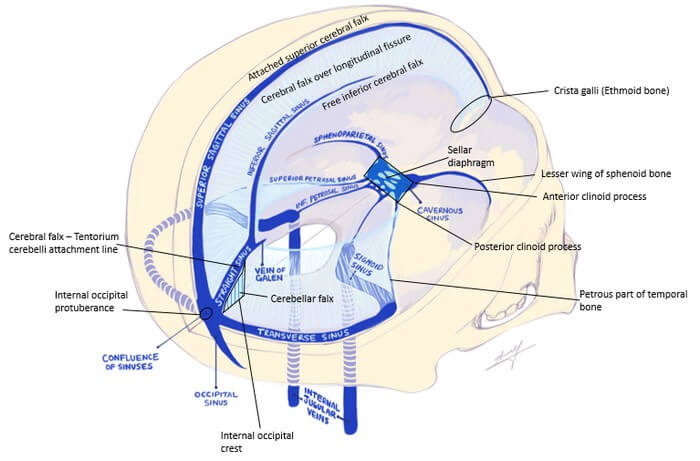
Falx cerebri (Cerebral falx): Extends from crista galli of ethmoid bone anteriorly to inner occipital protuberance posteriorly and projects over longitudinal cerebral fissure.
Falx cerebelli (Cerebellar falx): Extends from tentorium cerebelli superiorly to inner occipital protuberance inferiorly in the posterior cranial fossa.
Two horizontal reflections
Tentorium cerebelli (Cerebellar tentorium):
separates cerebellum and brainstem from cerebrum (occipital lobes)
attached to clinoid process anteriorly, upper edge of petrous temporal bone anterolaterally and to the occipital bone posterolaterally
falx cerebri is attached to the tentorium cerebelli and pulls it up – tent like appearance
Diaphragma sellae (Sellar diaphragm): Extends between anterior and posterior clinoid processes
partially covers the pituitary gland allowing the infundibulum and vessels
Dura is pain sensitive:
Dura is sensitive to pain, especially where it is related to the dural venous sinuses and meningeal arteries. Headaches can occur due to stimulation of the sensory nerve endings in the dura. It is innervated by all 3 divisions of the trigeminal nerve, sensory fibers of C2, C3 and meningeal branches of CN X and CN XII.
Epidural hematoma:
Rupture of high-pressure arteries (middle meningeal artery) running through the dura mater
Tearing of the dura separates bone and periosteal layer of dura creating an epidural space
“Lenticular” or “biconvex” in shape – the dural attachments provide more resitance to the collected blood to spread along than the underlying brain which get compressed
Doesn’t cross the suture line – hematoma is between the periosteal sublayer and the bone
Cross the dural reflections – hematoma is outside the periosteal sublayer
May have a lucid interval
Subdural or “Dural border” hematoma:
Shearing of low-pressure bridging veins is all that is necessary to create a subdural hematoma.
Subdural space is actually filled with the loosely arranged dural border cell sublayer. Pathologic bleeding into the border cell sublayer creates a subdural fluid space; otherwise, no true space actually exists.
“Crescent” shaped – the underlying brain provides more resistance to the collected blood than the loosely arranged dural border cells allowing it to spread along
Crosses the suture line as it is unaffected
Doesn’t cross dural reflections – pool at the site of dural reflections
Dural Venous Sinuses
1. Superior sagittal sinus: lies at the superior attached border of falx cerebri
Receives blood from superior cerebral veins (bridging veins) and emissary veins (connects extracranial venous system with intracranial venous sinuses – potention route of infection).
Receives CSF from arachnoid granulations.
2. Inferior sagittal sinus: lies at the inferior free border of falx cerebri
3. Straight sinus: lies at the line of attachment of falx cerebri and tentorium cerebelli
Formed by the union of inferior sagittal sinus and the great cerebral vein of galen.
4. Occipital sinus: lies in the attached border of tenorium cerebelli
Communicates inferiorly with the internal vertebral venous plexus.
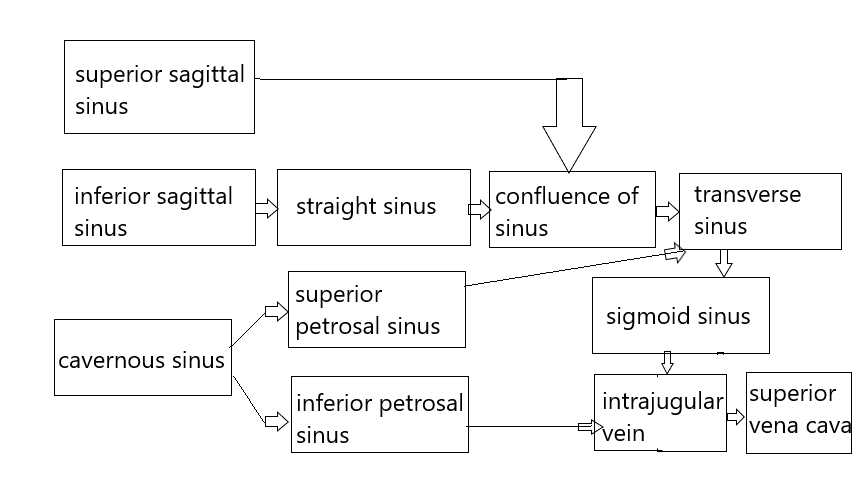
5. Confluence of sinuses (torcular Herophili): It is lies at the inner occipital protuberance and is formed by the union of:
Superior sagittal sinus
Straight sinus
Occipital sinus
It drains into the transverse sinuses.
6. Transverse sinuses: runs transversely at the posterolateral margin of tentorium cerebelli
Drains venous blood from transverse sinus into the sigmoid sinus.
Normally, one transverse sinus can be smaller than the other – usually the left is larger.
7. Sigmoid sinus: as the name suggests, it follows “S” shaped pathway – inferomedially from the transverse sinus (parietal to temporal bone) and then anterolaterally (temporal to occipital bone) into the jugular foramen where it continues as Internal Jugual Vein (IJV).
forms deep grooves in the bones along it’s course
8. Cavernous sinus:
The inter-cavernous sinuses lie on the body of sphenoid. These connect the cavernous sinuses of the 2 sides which sits on the side of the body of sphenoid.
It contains the siphon of Interncal Carotid Artery (ICA).
Receives venous blood from superior and inferior ophthalmic veins, superficial middle cerebral vein and sphenoparietal sinus.
Drains into superficial and inferior petrosal sinuses.
9. Superior petrosal sinus: runs along petrous part of temporal bone (anterolateral attachment of tentroium cerebelli)
Drains cavernous sinus into sigmoid sinus
10. Inferior petrosal sinus: runs in the groove between petrous temporal bone and basilar occipital bone
Drains cavernous sinus into sigmoid sinus
Basilar venous plexus: lies over the basilar part of occipital bone and connects the 2 inferior petrosal sinuses and communicates with the intervertebral venous plexus.
Dural Venous Sinus Thrombosis
Venous occlusion presents with a myriad of symptoms with variable severity. Sometimes the symptoms are as mild as simple headaches and other times they are severe enough to produce confusion, stupor, or even coma, along with paralysis and other focal neurologic deficits. Superior sagittal sinus or the dominant transverse sinus thrombosis can affect the arachnoid granulations absorption of cerebrospinal fluid, a consequently increase of cerebral swelling may occur. The subsequent venous hypertension can lead to oedema, and even hemorrhage.
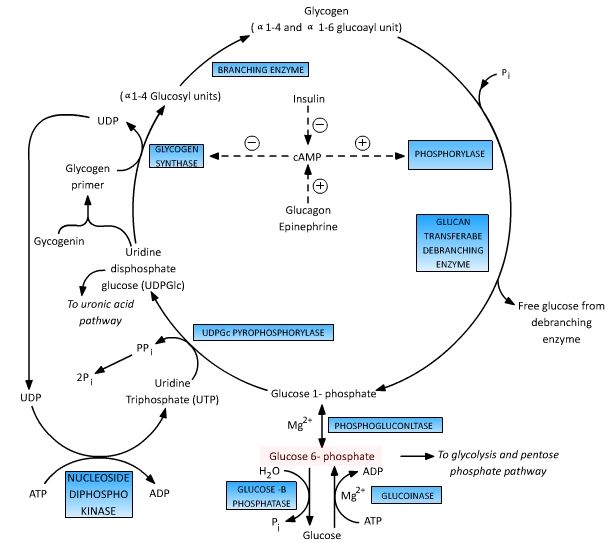
Glucose-6-Phosphate central to the 4 major metabolic pathways of glucose, i.e. glycolysis, gluconeogenesis, glycogenesis, glycogenolysis and HMP shunt (Pentose phosphate pathway). Glucose is immediately phosphorylated inside the cells to Glucose-6-Phsophate to trap them inside cell and prevent diffusion out of the cell. Glucose-6-Phosphate is the key intermediate to understand the…