Mechanical Axis Concept
- The primary mathematical goal is to obtain a straight load-bearing axis:
- Mechanical axis (MA) = line from femoral head center – to – center of knee – to – center of ankle
- MA of femur = 5-7° (average 6°) valgus to Anatomical Axis (AA) of femur
- AA of tibia = MA of tibia
- Neutral alignment = 180±3°
Natural Knee
- Not perfectly horizontal
- Joint line = around 3° varus
- Femoral joint line = 3° valgus (both distal and posterior joint lines) = 9° valgus to AA
- Medial femoral condyle > Lateral femoral condyle
- Tibial joint line = 3° varus = 3° varus to both MA and AA
- Femoral joint line = 3° valgus (both distal and posterior joint lines) = 9° valgus to AA
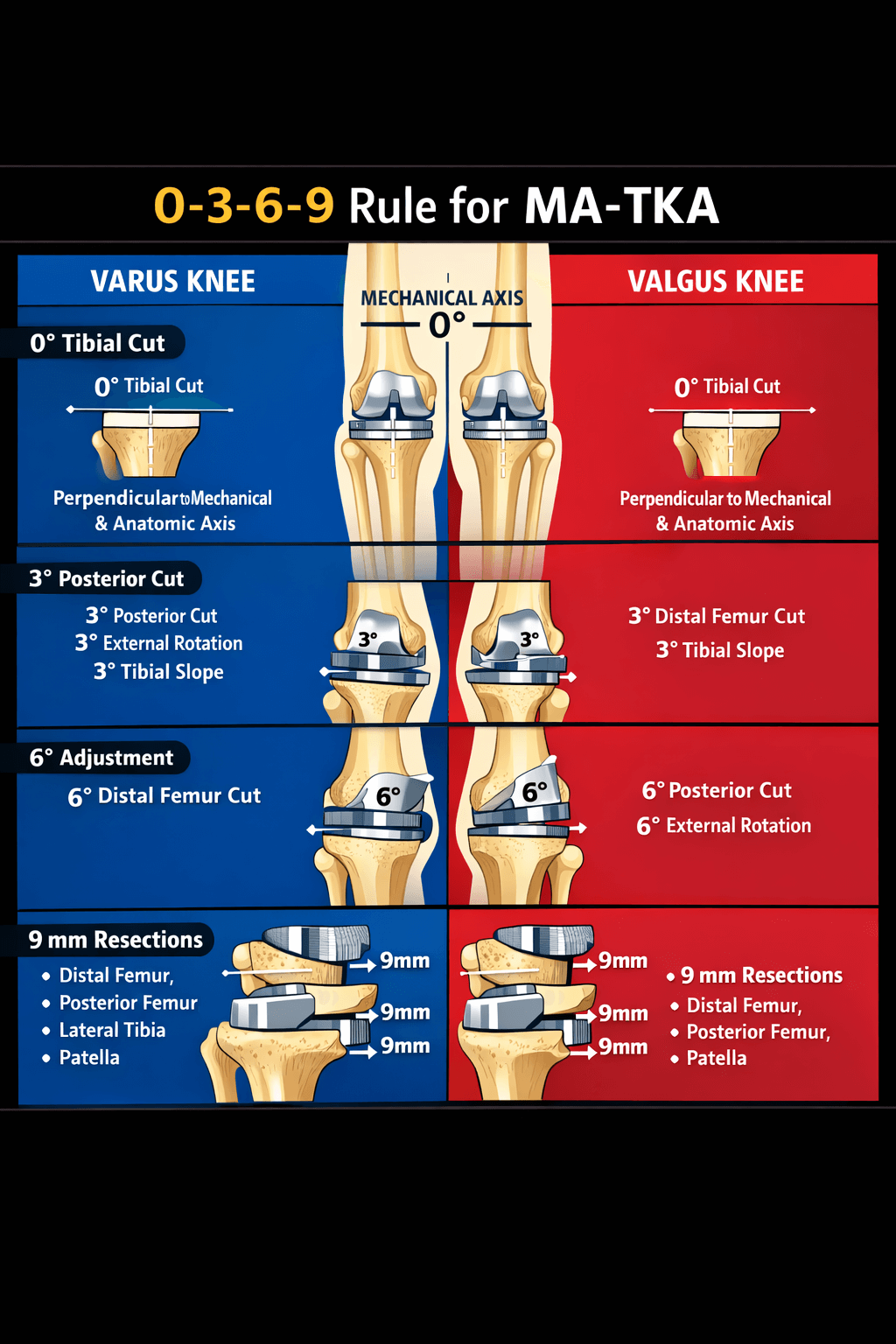
Target alignment in MA-TKA
- Tibiofemoral alignment restored to 6 ± 2° of anatomical valgus.
- Coronal plane:
- Femoral component = aligned between 5-10° of anatomical valgus
- Proximal tibia = resected at 90 ± 2° in relation to tibial shaft axis
- Sagittal plane:
- Femoral component = aligned between 0-10° of flexion
- Tibial component = neutral or slightly (5°) posterior slope
Tibial cut
- Affects both extension and flexion gap
- Extramedullary jig used = In line with MA and AA
- Cut = 90° to MA
- Joint line = 3° valgus relative to native joint-line (which is 3° varus)
- Posterior slope = 5°
Distal femoral cut
- Affects extension gap
- Intramedullary jig used = In line with AA
- Distal femoral cut angle = Valgus Correction Angle (VCA) = Femoral mechanical axis angle – Femoral anatomical axis angle
- Typical value: 5°–7° valgus relative to AA (average 6°)
- Joint line = 3° varus relative to native joint-line (which is 3° valgus)
Posterior femoral cut
- Affects flexion gap
- We know posterior femoral joint line also = 3° valgus normally
- But MA-TKA tibial cut = 3° valgus to native joint line
- So, to make a rectangular flexion gap:
- Posterior femoral cut = 3° external rotation to posterior condyle reference = Parallel to trans-epicondylar axis (TEA) = Perpendicular to Whiteside’s line
- This will cut more medial than lateral from posterior femoral condyle
- Posterior femoral cut = 3° varus to native joint line
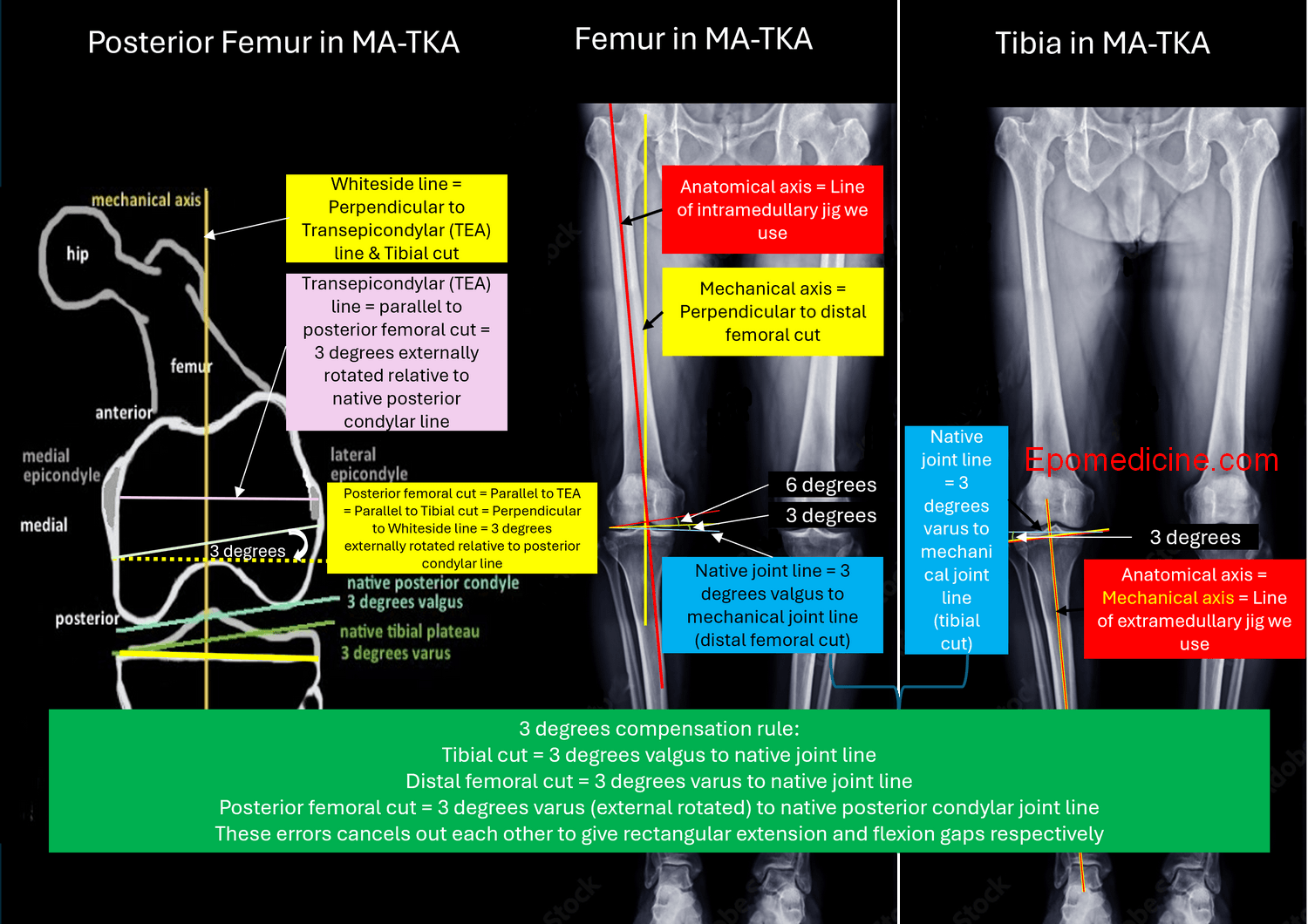
The 3° Compensation Rule
- Both cuts introduce small “errors” relative to native anatomy:
- MA-TKA Tibial joint line = 3° valgus from native surface
- MA-TKA Femoral joint line in both extension and flexion = 3° varus from native surface
- These cancel each other out to give:
- Parallel femoral and tibial joint line
- Perpendicular to the mechanical axis
- Extension gap = Flexion gap = Rectangular gap
Distal femoral and Tibial resection thickness = Implant thickness
- 8-10 mm from unaffected side
- Resection = Implant thickness – Cartilage wear
2 mm rule in TKA
- Gap balancing tolerance: Balanced knees require medial–lateral gaps ≤ 2 mm in extension and similar limits in flexion
- Tibial cut: 2 mm from more involved side
- Anterior femoral cut: 2-mm gap between the tip of the boom and the anterior cortex of
- the distal femur to prevent femoral notching
- Flexion and extension gap: Acceptable mismatch is upto 2 mm
- Joint line change: should be ≤ 2 mm (ideally <5 mm, but 2 mm is a precision target in modern TKA)
References:
- NATIVE KNEE ALIGNMENT — Hip & Knee Book
- Whiteside, Leo A. (2004). Ligament Balancing in Total Knee Arthroplasty || . , 10.1007/978-3-642-59295-9(), –. doi:10.1007/978-3-642-59295-9
- Mastering Orthopedic Techniques – TOTAL KNEE ARTHROPLASTY (First Edition: 2010)
- Elmasry SS, Sculco PK, Kia M, Kahlenberg CA, Cross MB, Pearle AD, Mayman DJ, Wright TM, Westrich GH, Imhauser CW. A geometric ratio to predict the flexion gap in total knee arthroplasty. J Orthop Res. 2020 Jul;38(7):1637-1645. doi: 10.1002/jor.24719. Epub 2020 May 25. PMID: 32410240; PMCID: PMC7345479.
- Bhor P, Pawar S, Kutumbe D, Vatkar A, Kale S, Jagtap R. Is Native Joint Line More Accurately Restored with Robotic Assisted Total Knee Arthroplasty than with Conventional Instruments? J Orthop Case Rep. 2025 Feb;15(2):233-238. doi: 10.13107/jocr.2025.v15.i02.5294. PMID: 39957945; PMCID: PMC11823860.

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.