60 year old smoker patient came with epigastric pain and shortness of breath for 4 hours. The patient was tachypneic with SpO2 90%. Other vital signs were relatively stable. ECG was done, Troponin I was positive and CK-MB was 100 IU/l.
What is there in ECG above?
ST elevation and Q waves in lead II, III and avF with reciprocal ST depression in lead I, aVL, V5 and V6 which indicates Acute inferior wall STEMI.
Presence of elevated ST segments, tall T waves and absence of T wave inversion points towards the acuteness of ischemia.
There is an abnormal Q in II, III, aVF diagnostic and specific for an inferior infarct of indeterminate age. Although Q is not deep (>1/3rd of R wave), it is wide > 1 box, signifying a pathological Q. Had the wide Q been isolated in lead III, the Q wave wouldn’t be considered pathological.
Abnormal Q waves:
Q wider > 1 box (0.04 sec) and deeper > 1 box in 2 contiguous leads.
Q of any width before the precordial transition zone (i.e., V1-V3).
Q may have a QS shape, which is a very wide and deep Q wave usually indicative of MI, except in leads III or V1 +/-V2 where it may be represent a normal variant.
Wide +/- tall R in V1 or V2 indicates posterior MI.
What to look for in ECG?
Mnemonic for ST Elevation: ABCD ELEVATION
- Angina (prinzmental or vasospastic)
- Brugada syndrome (RBBB like pattern and ST elevation in right precordial leads – susceptible to VT and sudden cardiac death)
- Class Ic antiarrhythmics
- DC cardioversion
- Electrolytes (hyperkalemia)
- Left bundle branch block (LBBB)
- Early repolarization
- Ventricular aneurysm
- Acute pericarditis
- Takotsubo cardiomyopathy and Trauma (myocardial contusion)
- Infarction (AMI)
- Osborne “J” waves (hypothermia)
- Normal variant (male pattern – majority have concave ST elevation ≥1 mm in precordial leads; most marked in V2)
Causes of ST elevation and a way to differentiate between various causes has been discussed here: http://epomedicine.com/medical-students/ecg-changes-in-pericarditis/
Diagnosis of STEMI in ECG
Definition of STEMI:
- New ST elevation at the J point in two contiguous leads of >0.1 mV in all leads other than leads V2-V3
- For leads V2-V3 the following cut points apply: ≥0.2 mV in men ≥40 years, ≥0.25 mV in men <40 years, or ≥0.15 mV in women
Other conditions which are treated as a STEMI
- New or presumed new LBBB
- Isolated posterior MI
The presence of reciprocal ST depression helps confirm the diagnosis.
Evolution of ECG in Acute MI
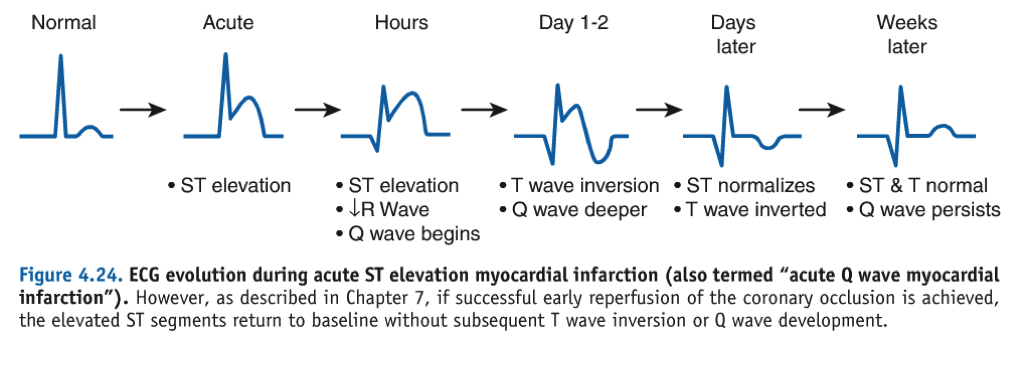
- T wave is the first to change and last to normalize:
- 1st – “T” goes up (hyperacute tall T waves)
- then – “T” goes down (T wave inversion)
- lastly – “T” comes to place (T wave normalizes)
- ST elevation:
- Appears after T wave goes up
- Normalizes before T wave normalizes
- Q wave:
- Appears after ST elevation
- Never returns to normal (persists) – also seen in old MI
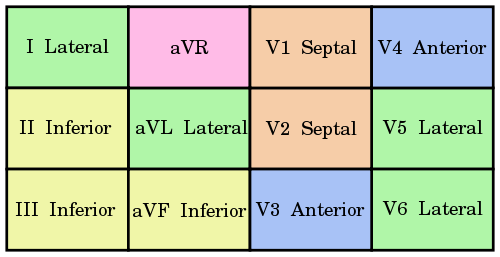
Localization of STEMI in ECG:
You really don’t need a mnemonic for this. Just remember that all the precordial leads are left-sided and hence, to detect the right sided infarction, we need to place the leads on right side of chest. As the precordial leads are placed sequentially to left, assign 2 precordial leads to each going from medial to lateral:
- V1 and V2: Septum
- V3 and V4: Anterior part of left ventricle
- V5 and V6: Lateral part of left ventricle
For limb leads: If you need a mnemonic for this, I have one –
- aVF (‘F‘ stands for floor i.e. inferior part of left ventricle)
- aVL (‘L‘ stands for lateral i.e. lateral part of left ventricle)
Do you remember this eithovein’s triangle?
The axis goes from negative to positive. Look how:
- Lead II and III shows inferior part
- Lead I shows anterior part
Reciprocal changes in STEMI: PAILS mnemonic
- Posterior ST Elevation – Anterior ST depression
- Anterior ST Elevation – Inferior ST depression
- Inferior ST Elevation – Lateral ST depression
- Lateral ST Elevation – Septal ST depression
- Septal ST Elevation – Posterior ST depression
In Right sided infarction, you see reciprocal changes in V1-V4.
Cardiac markers in Acute MI
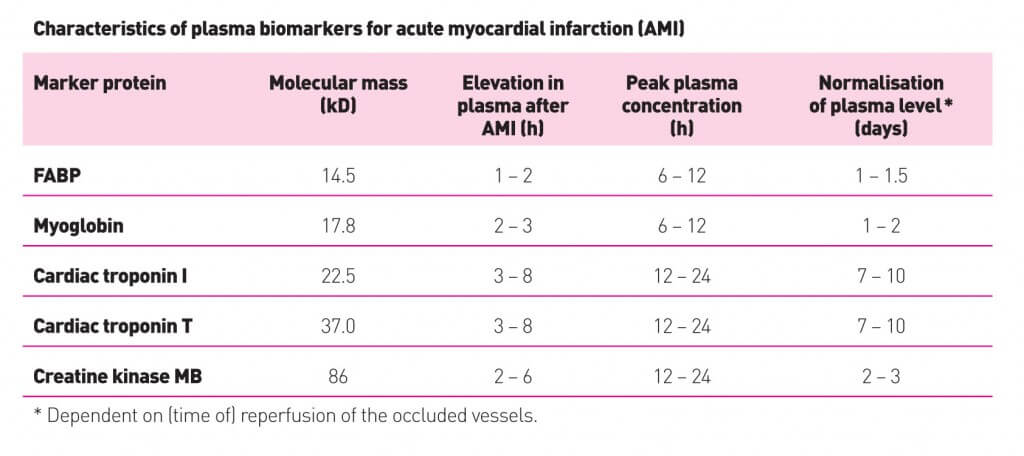 Time of appearance in sequence in AMI: Time to CALL 911
Time of appearance in sequence in AMI: Time to CALL 911
- Troponin I (Gold standard)
- CK-MB
- AST
- LDH
Note:
- Fatty acid binding protein (FABP) is the earliest marker of AMI (earlier than myoglobin).
- Troponin-I and CK-MB rises about the same time (no benefit of one over another for earlier detection).
- CK has 2 letters – rises as early as 2 hours and persists to 2 days (useful to detect reinfarction)
- TPnI has 3 letters – rises as early as 3 hours
- Troponin-I has 9 letters – persists upto 9 days
Causes of False Positive Troponin: CPRS
- Cardiac – failure, injury, pericarditis, cardiomyopathy
- Pulmonary embolism
- Renal failure
- Sepsis
Scoring of MI for mortality in first 14 days
Mnemonic: AMERICA (7 points)
- Age >65 years
- Markers – increased
- ECG – ST segment changes
- Risk factors – 3 or more (age, family history, diabetes, high cholesterol, hypertension, smoking, obesity, sedentary lifestyle, metabolic syndrome)
- Ischemia – 2 or more anginal events in last 24 hours
- CAD – prior 50% coronary stenosis
- Aspirin – use in last week
Point score:
- 0-1: 4.7%
- 2: 8.3%
- 3: 13.2%
- 4: 19.9%
- 5: 26.2%
- 6-7: 40.9%
What you need to do at Emergency room?
Immediate Managemet of Acute MI: MONARCH
- Morphine
- Oxygen
- Nitrates
- Aspirin
- Reperfusion (thrombolysis or PCI)
- Clopidegrol
- Heparin
What you need to be aware of in ICU?
Life-threatening complications of Acute MI: FEAR A MI
- Failure (heart failure)
- Effusion and tamponade
- Arrhythmia (AV block, VT)
- Rupture
- Aneurysm (ventricular)
- MI (Re-infarction)
What you need to send patient home with?
Overall treatment in Post-MI patients: ABCDE
- Aspirin, ACE inhibitors, Antianginals and Aldosterone antagonists (as per need of patient)
- Beta-blocker and Blood pressure control
- Cholesterol lowering and Cigarette stopping
- Diet and Diabetes control
- Education and Exercise
Review the pathophysiology of Ischemic heart dieasese here: http://epomedicine.com/medical-students/ischemic-heart-disease/

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.

Awesome👌👌👌👌
Thank you. You’ve just saved my morning. Thank you for taking the time to write such an amazing and practically useful contents 🙂
Muchas gracias, buenísimo aporte. <3