Synonyms: Radial pronator syndrome, Treatment resistant lateral epicondylitis (tennis elbow)
Anatomy of Radial Tunnel
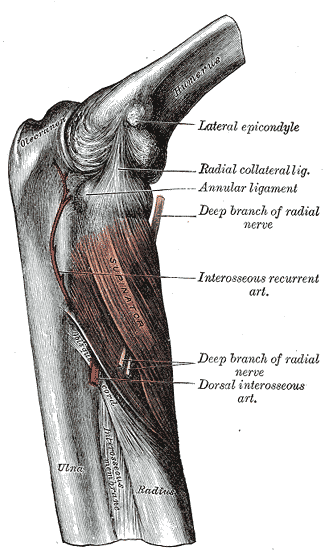
The anatomic radial tunnel (~5 cm) extends from the radial head to the inferior border of the supinator muscle.
Mnemonic: FREAS
- Fibrous bands anterior to radiocapitellar joint
- Radial recurrent vessels (leash of Henry)
- ECRB medial edge
- Arcade of Frohse (proximal aponeurotic edge of supinator)
- Supinator (distal edge)
Anatomic areas 1-3 may engage sensory area while 4-5 doesn’t.
Anatomically, the radial nerve emerges from the supinator and then becomes the PIN (Posterior Interosseous nerve). Deep branch of radial nerve (DBRN) courses through the supinator to exit as the PIN at approximately 7.5 cm distal to the Radio-humeral joint.
Diagnostic features
RTS may be confused with PIN syndrome but the main difference between the two is that RTS presents with sensory symptoms and any weakness is secondary to the pain while the PIN syndrome affects the motor portion of the nerve.
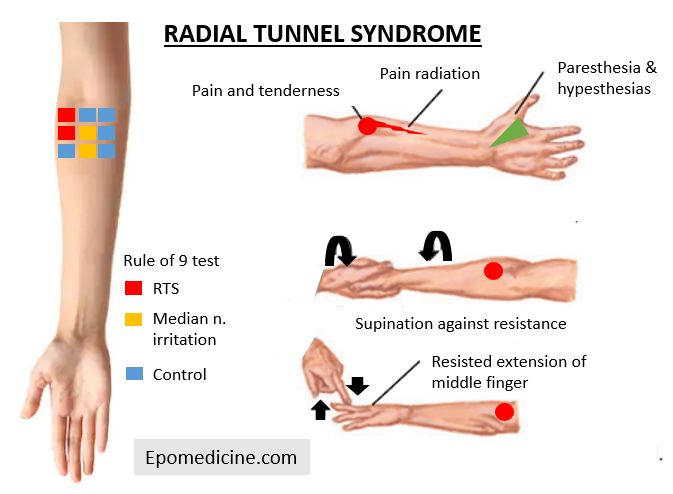
1. Patient may present with deep aching pain in dorsoradial proximal forearm which is worse at night and increases with lifting activities and forearm rotation and often accompanied by muscle weakness (due to pain rather than denervation).
2. Localized tenderness over the radial nerve 5 cm distal to lateral epicondyle.
3. Resisted long finger extension test – reproduces radial tunnel pain (some studies have considered as a pathognomic sign while in other studies there was no pain reproduction).
4. Resisted supination test – reproduces radial tunnel pain
5. Passive pronation with wrist flexion – passively stretches supinator muscle and increases pressure within radial tunnel to reproduce radial tunnel pain
6. Local anesthetic radial tunnel block – diagnostic if there is PIN palsy and pain is relieved.
7. Rule of Nine (RON) test – Subdivide the anterior, proximal forearm just distal to the elbow crease in to 9 regions arranged in a 3×3 grid. 3 medial regions without course of nerve are the control areas and expected to be free of pain and discomfort. Tenderness on the two proximal regions at the lateral column indicates radial nerve irritation. In the middle column, the two distal regions overlie the route of median nerve, and pain and tenderness in this area indicates a high level of median nerve irritation.
Reference: Moradi A, Ebrahimzadeh MH, Jupiter JB. Radial Tunnel Syndrome, Diagnostic and Treatment Dilemma. Arch Bone Jt Surg. 2015 Jul;3(3):156-62. PMID: 26213698; PMCID: PMC4507067.

{kind=link}