The anatomy of facial nerve has already been discussed in detail earlier. It is essential to have proper knowledge of anatomy to understand this section of clinical examination of facial nerve.
A) Inspection:
Observe:
- Face at rest for any facial asymmetry
- Any facial tics, symmetry of eye blinking or eye closure
- During smiling
In palsy:
- Blink: The eyelid on the affected side closes just a trace later than the opposite eyelid.
- Nasolabial folds: The weak one is flatter.
- Mouth: The affected side droops and participates manifestly less in speaking.
B) Motor function testing:
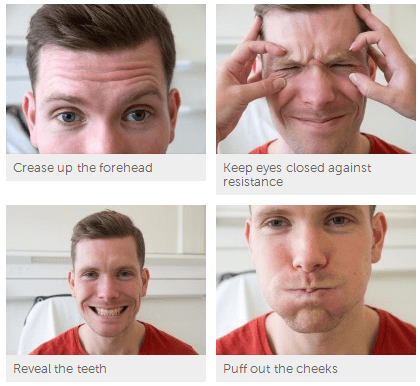
| Instruction | Muscle tested | Response in palsy |
| Ask the patient to wrinkle his/her forehead | Frontal belly of occipito-frontalis | Asymmetry as he/she cannot wrinkle his forehead on the side of palsy in LMN palsy |
| Ask the patient to close his/her eyes forcibly while you try to open the eyelids with your fingers | Orbicularis oculi | In LMN palsy eyelids don’t close completely. Instead the eyeball rolls up. This is known as Bell’s phenomenon. In healthy individuals, eyelids cannot be opened with mild force against patient’s resistance. |
| Ask the patient to show his/her teeth or smile | Levator anguli oris, Zygomatic major and minor, Depressor anguli oris, Buccinator, Risorius | Angle of mouth deviates towards normal side |
| Ask the patient to blow out cheeks with mouth closed i.e puff the cheeks and assess power by your attempt to deflate the cheekAsk the patient to whistle | Orbicularis oris, Buccinator | Patient can’t blow out his cheek as air escapes from affected side |
| Ask the patient to clench his/her teeth and simultaneously depress the angles of mouth | Platysma | Folds of platysma is seen in the neck as platysma contracts |
C) Sensory function testing (Taste test):
- Explain the procedure to patient and instruct him/her not to speak during the procedure
- Give the patient cards indicating various tests to be tested and instruct him/her to signal by showing the card for the taste perceived
- Ask the patient to protrude out his tongue
- Place sweet, salt, bitter and sour taste solutions on one side of tongue one by one using cotton-bud
- Patient should be asked to rinse his/her mouth after test for each taste
- Test the opposite side also
Other tests (usually not done):
- Corneal reflex (Afferent is by trigeminal nerve while efferent is by facial nerve)
- Schirmer’s test (Secretomotor function)
You may need to:
- Inspect external auditory meatus – Herpes zoster Oticus (Ramsay hunt syndrome)
- Ask if there has been any hearing changes? – facial nerve supplies stapedius – paralysis results in hyperacusis
Differentiating UMN (Supranuclear) and LMN (Nuclear and Infranuclear) Facial nerve palsy:
| UMN type | LMN type | |
| Facial motor function | Wrinkling of forehead preserved (frontalis unaffected) | Total face is involved |
| Bell’s phenomenon | Absent | Present |
| Facial muscles | Not atrophied | Fascicultions, Atrophied |
| Taste sensation | Preserved | May be lost |
| Corneal reflex | Preserved | Lost |
| Hemiplegia | Contralateral | Ipsilateral |
| Babinski reflex | Present | Absent |
Causes of Unilateral and Bilateral Facial Palsy:
1. Unilateral facial palsy: Ramsay hunt syndrome, Acoustic neuroma, Meningioma, Cholesteatoma, Traumatic injury
2. Bilateral facial palsy: Poliomyelitis, Leukemia, Melkersson syndrome, Mobius syndrome, Myasthenia gravis, Myotonic dystrophy
3. Can cause either unilateral or bilateral palsy: Bell’s palsy, Otitis media, Parotid disease, HIV, Leprosy

Can the eyes closed in UMN 7th nerve palsy?
Yes, the eyes can be closed in upper motor neuron lesion of facial nerve.
Upper part of the face have bilateral representation…
Is hemiplegia ipsilateral in UMN lesion?
Thank you for pointing out, the correction has been made. Look at this figure to understand – http://epomedicine.com/medical-students/applied-anatomy-of-facial-nerve/#Supranuclear_pathways
While the upper face receives bilateral UMN innervation, the lower face receives only contralateral UMN innervation. Hence, there is contralateral facial nerve palsy.
It’s helping me alot
damn i am happy with the description link. can someone explain why every infranuclear lesion dont cause facial paresis upto stylomastoid foramen?.
Ent omf and head neck ca resident 2nd year. bhilai C.G.
The signs and symptoms of infranuclear lesions differ based on the site of the lesion:
At or just above the stylomastoid foramen: It causes Bell’s palsy which presents as loss of motor functions of all muscles of facial expression resulting in the deviation of mouth toward the normal side, inability to shut the mouth and eye and accumulation of food in the vestibule of mouth flattening of expression lines.
Above the origin of chorda tympani: Bell’s palsy plus reduced salivation and reduction of taste sensations in the anterior two-third of the tongue.
Above the origin of nerve to stapedius: Additionally hyperacusis
At the geniculate ganglion: Additionally reduction in lacrimation
Found this while looking up what my neuro-ophthalmologist was talking to me about. I have Idiopathic Intracranial Hypertension, and it’s affecting not only the 7th cranial nerve, but others as well. Symptoms are definitely not as severe or noticeable to most people, I’m kinda just stuck with “resting bitc# face” because it takes a lot more effort to move the left side of my face, so most facial expressions i look really indecisive or confused and. I wouldn’t fit in either of the 2 categories, my answers are all over the chart, and IIH wasn’t listed in possible causes. If my regular doctor had known any of this, maybe It wouldn’t have permanently affected my vision so much. Hope it helps someone.
Interesting information
can you tell at same time of clinical test the branch tested
l am belly’s palsy patient about one month what should I do to recover from this facial nerve.
I was told I have Bell’s Palsy, literally seven months ago and is still suffering from BP. With this condition comes with drooping left side of the face and my left eye couldn’t close entirely. My left ear was sensitive to sound the first four months. I have been experiencing severe headache affecting the left side of the head, pain and stiffness in the neck for months. As I thought my was progressing, I experience neurological pain and aches that throbs and wouldn’t go away. The pain seeps and elicits burning sensations to my entire face, neck and sporadic pain down my back. My left eye continues to twitch uncontrollably. I am in constant, excruciating pain and the dr. prescribed me gabapentin which seems to not do much. Could someone please share their knowledge and expertise that my condition is solely Bell’s Palsy and not anything else. Thank you in advance =)
From the description, the lesion seems to be infranuclear and above the level of nerve to stapedius. Tingling sensation, pain, twitching, etc. may be the signs of recovery as the nerves are growing. Mixing up of nerve wirings may lead to synkinesis and recovery may take longer in such cases.
What is the difference between supranuclear and infranuclear facial nerve palsy clinically and anatomically?
Supranuclear and Infranuclear facial nerve palsy has been explained here: https://epomedicine.com/medical-students/applied-anatomy-of-facial-nerve/