Synonym: Necrotizing papillitis
In renal papillary necrosis, part or all of necrotic renal papilla sloughs and may fall into the pelvicalyceal system, which may remain there (and get calcified) or may be voided down the ureter (often causing obstruction). The renal medulla and papillae are vulnerable to ischemic necrosis because of peculiar arrangement of their blood supply and hypertonic environment.
Common causes of papillary necrosis
Remember the mnemonic: POSTCARDS
-
Pyelonephritis
-
Obstruction of the urinary tract
-
Sickle cell hemoglobinopathies, including sickle cell trait
-
Tuberculosis
-
Cirrhosis of the liver, Chronic alcoholism
-
Analgesic abuse
-
Renal transplant rejection, Radiation
-
Diabetes mellitus (commonest – accounts for more than 50% of the cases of renal papillary necrosis 1)
-
Systemic vasculitis
Best modality of evaluation of papillary necrosis
IVU or retrograde pyelography
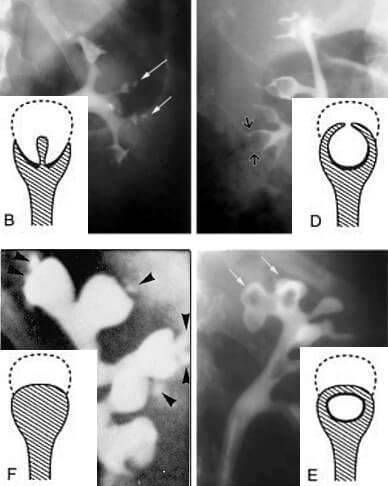
Radiological signs of papillary necrosis
If the papillary sloughing is:
- Partial: Contrast tracks around or onto it
- Complete: Calyx appears spherical (with loss of papillaryindentation) and as filling defect
appearance (B), Forniceal excavation (C), Lobster
claw appearance (D), Signet ring appearance (E),
and sloughed papilla with clubbed calix (F)
Ball-on-tee appearance: Contrast material filling central excavations in the papilla of the interpolar region gives ball-on-tee appearance.
Lobster claw sign: Excavation extending from the caliceal fornices produces the lobster claw deformity.
Signet ring sign: The necrotic papillary tip may remain within the excavated calyx, producing the signet ring sign when the calyx is filled with contrast material.
Club shaped saccular calyx: Due to sloughed papilla

Really very informative and consize