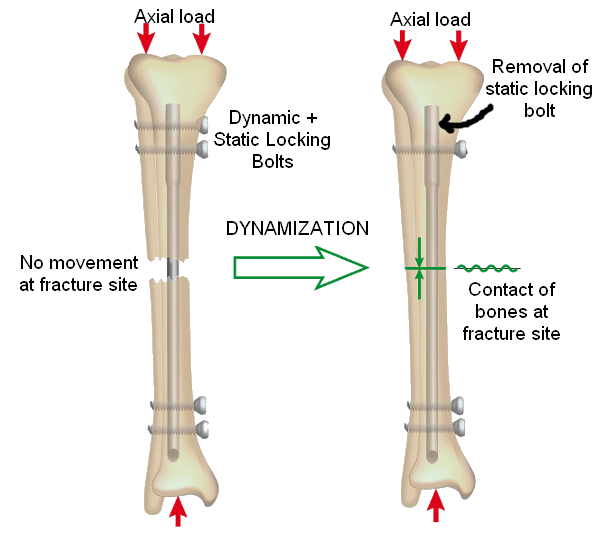
Dynamization of intramedullary nail is the process of converting a static interlocking nail (provides better fixation & rotational control) to a dynamic locking nail (allows axial loading of fracture to stimulate bone healing). Dynamization converts a bridging mode of fixation to the splinting mode.
- Static locking: nail is locked on both cortices using screw, so that there is no relative movement between bone and nail
- Dynamic locking: nail is locked only on distal cortex using screw and the nail will just telescope through the proximal medulla till the fracture fragments are brought together
Timing of Dynamization: Dynamization should be performed when the fracture and the newly formed callus have gained enough stability to withstand axial forces without collapse, usually 2-3 months after the initial fixation. If there is any inherent risk of shortening, dynamization should be postponed.
Indication of Dynamization: It is no longer a standard practice to dynamize the statically locked intramedullary nail if the healing is progressing normally. It is indicated when there is delay in healing and there is risk of development of nonunion or in cases of established pseudoarthrosis.
Technique of Nail Dynamization:
1. Removing the proximal static locking screw (In nails with dynamic slots): In modern nails, there are 2 proximal slots – oval one for dynamic locking and round one for static locking. Removing the static locking screw proximally will allow the proximal fragment to telescope under the limits allowed by dynamic (oval) slot while providing rotational stability which is usually adequate for bone contact.
2. Removing the screws from longer segment or farthest from fracture (In nails with only static slots): Screws are removed from longer segment to maintain adequate control of the shorter fragment.
Associated risk of dynamization: Premature dynamization may cause shortening, instability and non-union.
References:
- The elements of fracture fixation, 4th edition – Anand J Thakur
- Diagnostic imaging of musculoskeletal diseases – Akbar Bonakdarpour, William R. Reinus, Jasvir S. Khurana
- Current Practice of Fracture Treatment – P.C. Leung

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.