Enneking (MSTS) Staging for Malignant Bone Tumors
| Stage | Grade | Site | Metastasis |
| IA | Low | Intra-compartmental | None |
| IB | Low | Extra-compartmental | None |
| IIA | High | Intra-compartmental | None |
| IIB | High | Extra-compartmental | None |
| III | Any | Any | Regional or Distant |
A compartment is defined as “an anatomic structure of space bounded by natural barriers of tumor extension.” Intra-compartmental lesions are easier to delineate clinically, surgically, and radiographically than Extra-compartmental lesions and have a correspondingly higher chance of adequate removal without amputative procedures.
For spinal column tumors, the Enneking classification does not take into account the presence of a continuous epidural compartment, the neurologic implications, and the need for restoring spinal stability.
Grading of Sarcomas
Grade I:
- Low grade intramedullary osteosarcoma
- Parosteal osteosarcoma
- Osteo-fibrous dysplasia-like adamantinoma
- Clear cell chondrosarcoma
Grade II:
- Periosteal osteosarcoma
- Classic adamantinoma
- Chordoma
Grade III:
- Osteosarcoma (conventional, telangiectatic, small cell, secondary, high-grade surface)
- Undifferentiated high-grade pleomorphic sarcoma
- Ewing sarcoma
- Dedifferentiated chondrosarcoma
- Mesenchymal chondrosarcoma
- Dedifferentiated chordoma
- Malignancy in giant cell tumor of bone
- Angiosarcoma
Variable:
- Conventional chondrosarcoma (grade 1-3 according to Evans)
- Leiomyosarcoma of bone (grade 1-3 according to FNCLCC)
Enneking (MSTS) Staging for Benign Bone Tumors
| Stage | Definition | Biological behavior | Soft tissue tumor example | Bone tumor example |
| 1 | Latent | Remains static or heals spontaneously | Lipoma | Nonossifying fibroma |
| 2 | Active | Progressive growth, limited by natural barriers | Angiolipoma | Aneurysmal bone cyst |
| 3 | Aggressive | Progressive growth, invasive, not limited by natural barriers | Aggressive fibromatosis | Giant cell tumor |
AJCC staging for Malignant Bone Tumors
| Stage | Grade | Size | Metastasis |
| IA | Low | <8 cm | None |
| IB | Low | >8 cm | None |
| IIA | High | <8 cm | None |
| IIB | High | >8 cm | None |
| III | Any | Any | Skip metastases |
| IVA | Any | Any | Lungs |
| IVB | Any | Any | Regional lymph nodes or another distant site (non-pulmonary) |
AJCC staging for Soft tissue Sarcomas
| Stage | Grade | Size | Metastasis |
| IA | Low | <5 cm | None |
| IB | Low | >5 cm | None |
| II | High | <5 cm | None |
| IIIA | High | 5-10 cm | None |
| IIIB | High | >10 cm | None |
| IV | Any | Any | Regional lymph node or distant metastases |
Campanacci staging (Radiological) for Giant Cell Tumor
Grade 1 – Intramedullary lesion confined to bone
Grade 2 – Thinned, expanded cortex
Grade 3 – Cortical breakout
Evans Histological Grading for Chondrosarcoma
Grade I – low cellularity, limited cytonuclear atypia, few multinucleated cells, a mainly chondroid matrix and the absence of mitoses
- 90% 5 year survival
Grade II – increased cellularity, and increased muco-myxoid degeneration of the matrix; moderate cytonuclear atypia and occasional mitoses
- 80% 5 year survival
Grade III – chondrosarcomas are highly cellular, with nuclear polymorphism, mitoses and a mostly myxoid matrix
- 30% 5 year survival
Reference: Evans, H. L., Ayala, A. G., & Romsdahl, M. M. (1977). Prognostic factors in chondrosarcoma of bone.A clinicopathologic analysis with emphasis on histologic grading. Cancer, 40(2), 818–831. doi:10.1002/1097-0142(197708)40:2<818::aid-cncr2820400234>3.0.co;2-b
Weinstein-Boriani-Biagini (WBB) Classification for Primary Spinal Tumors
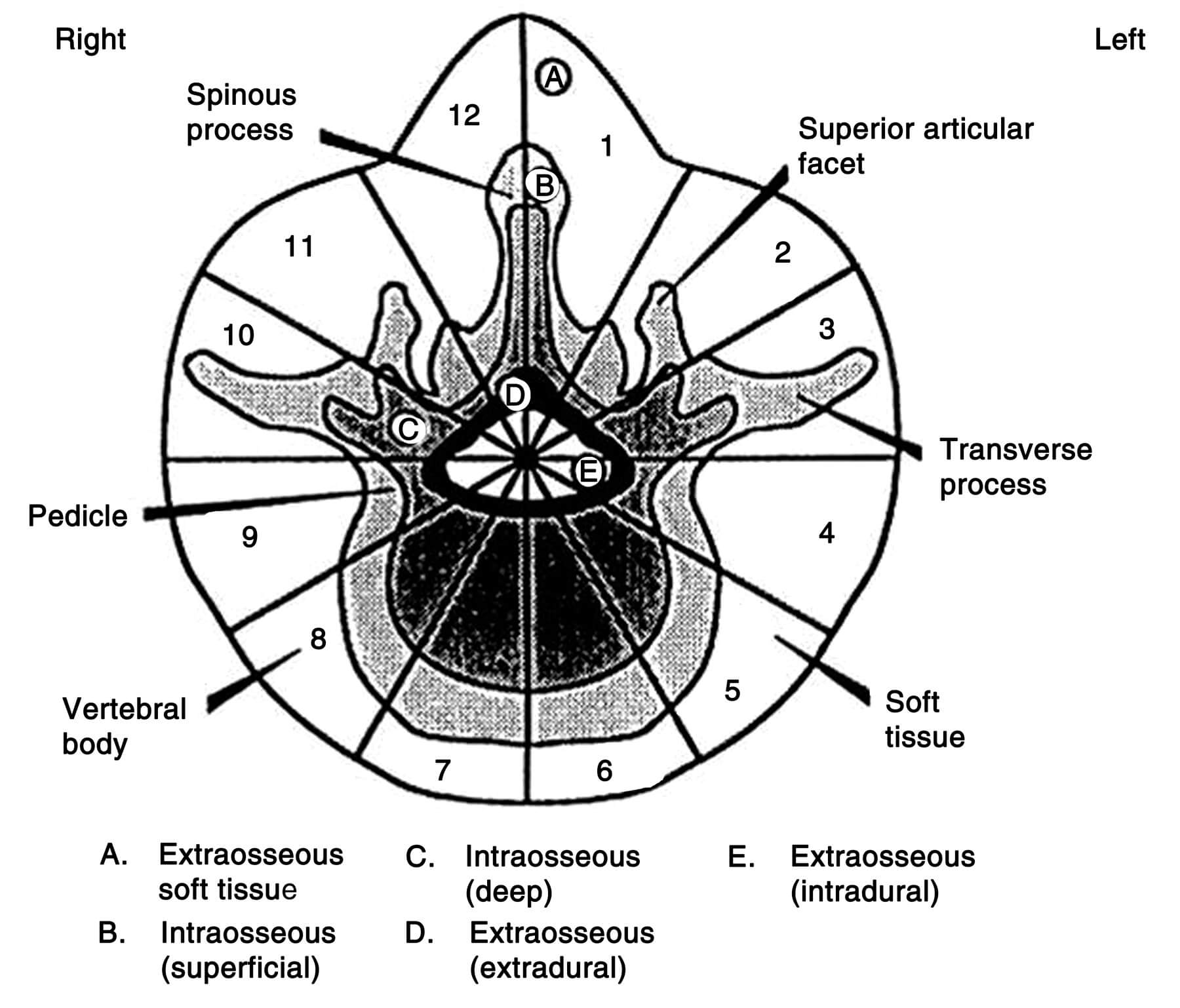
The WBB surgical staging system describes the involvement of a specific vertebra in terms of sectors involved, arranged clockwise in 12 sectors on an axial vertebral face from the left side of the spinous process (1) to the right side of the spinous process (12). The tumor is further divided into five concentric layers of tissue penetration centered about the dural sac:
- A— Extra-osseous soft tissue
- B — Intraosseous superficial
- C — Intraosseous deep
- D — Extraosseous (extradural)
- E — Extraosseous (intradural)
Procedure required according to zone:
- 4-8 or 5-9: Vertebrectomy (double approach)
- 2-5 or 7-11: Sagittal resection (double approach)
- 10-3: Posterior arch resection (posterior approach)
Surgical Margins according to Enneking Staging
| Enneking Stages | Margin for Control |
| Benign | |
| 1 | No management unless for decompression or stabilization |
| 2 | Intralesional excision ± local adjuvants |
| 3 | Marginal en-bloc excision |
| Malignant | |
| Ia | Wide en-bloc excision |
| Ib | Wide en-bloc excision |
| IIa | Wide en-bloc excision + effective adjuvants |
| IIb | Wide en-bloc excision + effective adjuvants |
| III | Palliative |
Surgical margins according to plane of surgical dissection:
- Intralesional: Tumor
- Debulking
- Curettage:
- Simple – creating a cortical window and ‘scooping out’ the underlying tumor
- Extended – use of adjuvants such as liquid nitrogen, phenol, polymethylmethacrylate, or thermal cautery
- Marginal: Reactive zone or Pseudo-capsule
- Wide: Normal tissue
- Radical: Entire involved compartment