| Site | Point of insertion | Direction | Indications |
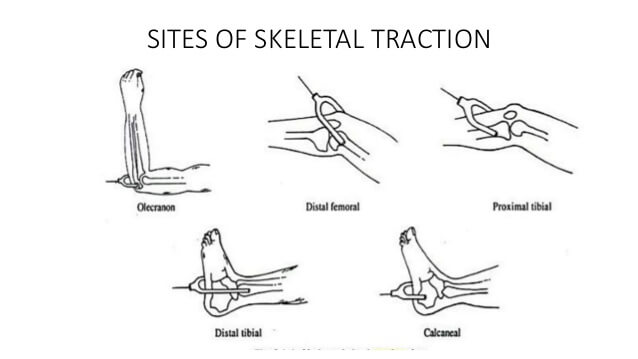
| Olecranon (K-wire) | 1.25 inches (3 cm) distal to olecranon tip – deep to subcutaneous border of upper ulna (avoids ulnar joint and open epiphysis) | Medial to Lateral – At right angles to longitudinal axis of ulna (Avoids ulnar nerve) | Supracondylar or Distal humerus fractures |
| 2nd and 3rd metacarpals (K-wire) | 1 inch (2-2.5 cm) proximal to distal end of 2nd metacarpal | Radial to ulnar, traversing 2nd and 3rd metacarpal diaphysis – At right angles to the longitudinal axis of radius | Difficult reduction forearm or distal radius fracture |
| Greater trochanter (Steinmann or Denham’s pin) | 1 inch (2.5 cm) below the most prominent part of greater trochanter – midway between anterior and posterior surface of femur | Lateral to Medial | Central fracture dislocation of hip |
| Distal femur (Steinmann or Denham’s pin) | 3 cm proximal to lateral joint line (i.e. just proximal to femoral condyle or at the level of proximal pole of patella in relaxed and extended knee) – avoids lateral knee joint capsule which reaches 1.25-2cm above knee joint, distal femoral physis | Lateral to Medial – pin should pass along or slightly posterior to the midcoronal plane of femoral shaft and pass just proximal to the adductor tubercle in order to avoid engagement of the collateral ligaments (Traditionally medial to lateral direction suggested to save femoral artery in Hunter’s canal) | Superior force acetabular fractures and femoral shaft fractures |
| Proximal tibia -Perkin’s traction (Steinmann or Denham’s pin) | 2cm behind and 2cm below tibial tuberosity (to avoid proximal weaker cancellous bone and to avoid common peroneal nerve distally as it courses anteriorly after winding around fibular nerve) | Lateral to Medial (to avoid common peroneal nerve) | Fractures of tibia and femur from subtrochanteric region distally |
| Distal tibia | 5cm above the ankle joint – midway between anterior and posterior borders of tibia | Medial to Lateral (avoid saphenous vein) | Tibial plateau fracture |
| Calcaneus | 1.5 inches (4 cm) inferior and posterior to medial malleolus (avoid tendons, neurovascular bundle passing behind the malleoli and subtalar joint) | Medial to Lateral | Tibial shaft fracture or calcaneal fracture |
How to should set Patient position for end of distal femur fracture?Please.
For the distal femur fracture, proximal tibial traction (Perkin’s traction) would be appropriate if planned for skeletal traction. The pull on the femur should be in line with it’s axis (the pulley should be adjustable accordingly; up and down) and the weight must be enough to correct the length and reduce the fracture. 10% of body weight can be used for maintenance traction. The distal fragment has tendency for posterior displacement due to pull of gastrocnemius, hence to prevent this the thigh should be supported on a firm triangular foam wedge, or by folded pillows or more appropriately Bohler Braun splint. The angle of the padded frame is pushed proximally to support the distal fragment.
Length and rotation must be checked daily. If required, length adjustment can be done by increasing or decreasing the weight used for traction. Rotation and maintenance of dorsiflexion in the ankle can be achieved by applying an adhesive sock to the forefoot with a cord over a pulley on the Balkan beam. This pulley should be adjustable from side to side to control rotation.
Check X-ray must be done weekly for 1st 4 weeks if possible, then 4 weekly to monitor for progress of bone healing.
You can check the pictures and detailed description here: https://surgeryreference.aofoundation.org/orthopedic-trauma/adult-trauma/distal-femur/extraarticular-fracture-simple/traction#skeletal-traction