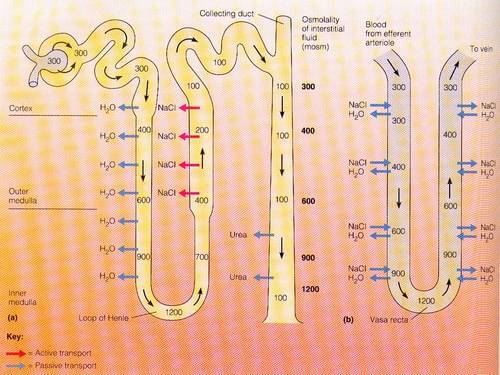
The term counter-current means flow in opposite direction. The renal counter-current mechanism comprises of:
- Flow of filtrate in opposite direction in nephron loop (down the descending limb and up the ascending limb of LOH or Loop of Henle) – that functions as a counter-current multiplier
- Flow of blood in opposite direction in vasa recta (down one side and up another) – that functions as a counter-current exchanger
Osmolarity refers to the saltiness of a solution. The saltiness of a solution increases either by removal of water or addition of salt.
Descending limb of LOH has thinner membrane – permeable to water and urea but not salt.
Ascending limb of LOH has thicker membrane – impermeable to water as well but has pump to transport salt out actively.
Distal collecting duct (CD) is permeable to urea but not water.
Vasa recta is freely permeable to both solute and water throughout the length. Water diffuses along the osmotic gradient and NaCl diffuses along its concentration gradient.
Counter-current multiplier
Multiplier = Increases the salt concentration of medulla (this allows the collecting tubule to reabsorb water via osmosis, thereby concentrating the urine)
- Ascending limb of LOH pumps salt out into ECF making it more salty.
- Filtrate entering the nephron loop is less salty like blood (300 mOsm/kg). Hence, water leaves the Descending limb of LOH into saltier ECF making filtrate also more salty.
- As, the salty filtrate move up the ascending limb of LOH, salt is actively transported out into ECF making it more salty. So, when a fresh filtrate flows into nephron, it loses water into more salty ECF.
- So, this loop configuration creates a cortico-medullary osmotic gradient of 300-1200 mOsm/kg, i.e. medulla is always saltier than cortex.
Mnemonic: Remember, the salty water sinks deeper.
Counter-current exchanger
Exchanger = Water is exchanged for salt along the vasa recta to maintain the gradient created by multiplier system (if there would be no counter-current system in vasa recta, the salt would be carried away by vasa recta and the gradient would be lost)
As the ECF is saltier as we go deeper:
- As blood flows down the vasa recta, blood loses water and takes salt making it more saltier.
- As the saltier blood flows up the vasa recta, blood takes water and loses salt
Intra-renal urea recycling
Recycling = Urea gets out of distal CD to get in descending limb of LOH which is subsequently brought back to distal CD; It is also recycled in vasa recta (hence, urea is not lost).
Recycled urea helps to make the ECF saltier contributing to the medullary concentration gradient.
Osmolalities (Saltiness) at different points in the tubule
Renal interstitial osmolality values:
- Cortex osmolality: 300 mOsm/kg
- Outer medulla: 800 mOsm/kg
- Inner medulla: 1200 mOsm/kg
Loop of Henle osmolality values:
- Proximal tubule, straight part: 300 mOsm/kg
- Descending limb: 800 mOsm/kg
- Hairpin turn: 1200 mOsm/kg
- Ascending thin limb: 800 mOsm/kg
- Ascending thick limb: 100 mOsm/kg, at the end
Osmotic Equilibrating Device
1. When ADH plasma levels are increased during negative water balance:
The collecting ducts become highly permeable to water and water moves out of the collecting duct into the hyperosmotic medullary interstitium down its chemical gradient until the collecting duct lumen and corresponding medullary interstitium have equal water concentrations. So much water leaves by the end of the collecting duct that urine volume is low (perhaps 500 ml/day) and the urine osmolality is high (~ 1200 mOsm/L). The kidneys have saved volume.
2. When ADH plasma levels are decreased during positive water balance:
Water is trapped in the collecting ducts and some solute removal still occurs in the collecting ducts; therefore a very large volume of dilute urine (upto 100 mOsm/L) is formed.