Origin and Spread of Cardiac Impulse
Mnemonic: SAIL MRS. SAVE APPS

1. SA node (generates impulse at highest rate, i.e. 70-80/min)
3 Internodal pathways:
- Anterior internodal fiber of Bachman
- Middle internodal fiber of Wenckebach
- Posterior internodal fiber of Thorel
2. AV node
Bundle of His
3. Interventricular septum – Left
4. Midportion Right Septal activation
Purkinje System
5. Septum (upper to lower) – purkinje system
6. Apex
7. Ventricular wall – Endocardium to epicardium
Epicardial surface of right ventricle is depolarized earlier than left because of its thinner wall.
9. AV groove
10. Posterobasal portion of left ventricle, Pulmonary conus and Septum (uppermost portion) – last part of heart to be depolarized
Conduction velocity of cardiac tissue
Mnemonic: Park At Ventura South Avenue (from fastest to slowest)
- Purkinje fibers (4 m/s – fastest)
- Atrium, interatrial and internodal tract (1 m/s)
- Ventricles (<1 m/s)
- SA node (0.05 m/s – 2nd slowest)
- AV node (0.02-0.05 m/s – slowest)
SA node and AV node lack functioning fast channels (Na+ channels) that open and closes quickly. Due to this reason, the depolarization is slow in these tissues and are regarded as slow fibers.
The action potential in SA node and AV nodes are due to Calcium with no contribution by sodium influx.
Resting membrane potential is much more negative (-90 mV) in ventricular muscle fibers instead of -55 mV in nodal fibers. At the less negative (-55 mV) RMP of nodal fibers the fast Na+ channels mainly have already become inactivated. Therefore, only the slow Na+ channels can become activated and cause action potential. Hence, the action potential is slower.
Pacemaker potential
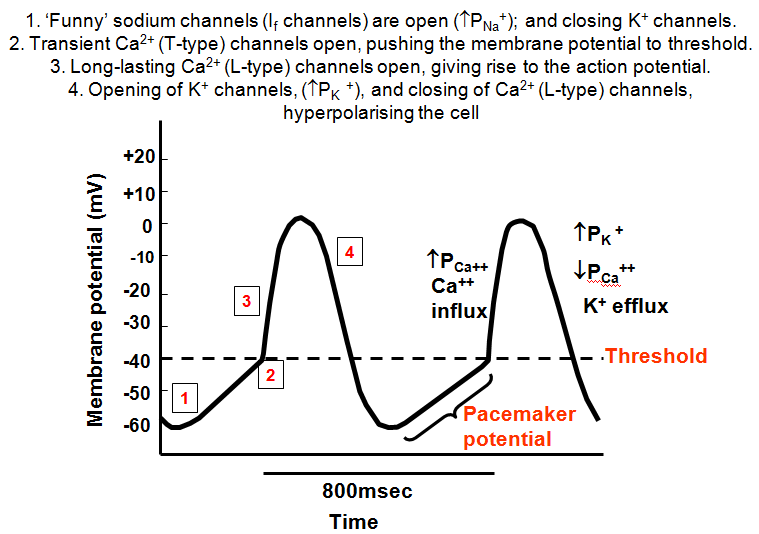
| Phase | Description | Mnemonic | Mechanism |
| 0 | Depolarization | Climb | Calcium influx |
| 3 | Repolarization | Plummet | Potassium efflux |
| 4 | Resting potential | Funny sodium channels – sodium influx |
Cardiac Action Potential
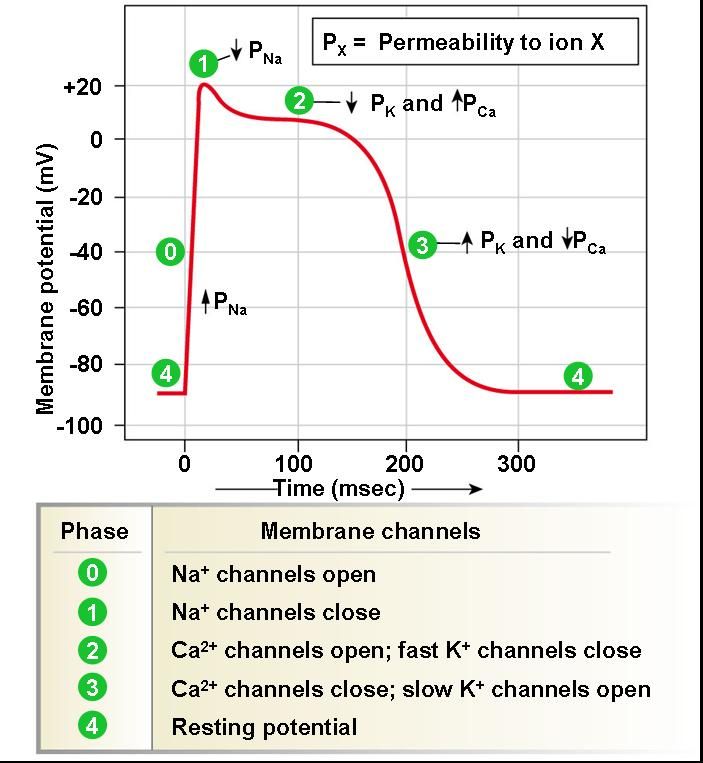
| Phase | Description | Mnemonics | Mechanism and Events |
| 0 | Rapid depolarization | Summit | Sodium influx (rapid) |
| 1 | Early repolarization | Plummet | Potassium efflux (fast) |
| 2 | Plateau | Continue | Calcium influx (slow) |
| 3 | Final repolarization | Plummet | Potassium efflux (slow) |
| 4 | Resting potential | Na+/K+ ATPase – slow entry of sodium into cell until threshold potential is reached. |
Cardiac contraction
After depolarization via sodium channels, calcium enters the cardiomyocyte via L-type calcium channels which are in close contact with ryanodine receptors in sarcoplasmic reticulum via T-tubules. Calcium activates ryanodine receptors (RyR) which triggers calcium release from sacroplasmic reticulum.
Calcium binds to troponin C which brings confirmational change in tropomyosin and exposes active site between actin and myosin. Myosin head interacts with actin and ATP hydrolysis leads to cross-bridge formation. After power stroke, actin is released with ATP binding to myosin.
L-type calcium channels inactivate towards the end of phase 2 leading to calcium influx arrest. Calcium induced calcium release from sarcoplasmic reticulum is stopped. At the same time, calcium is sequestered back into the sarcoplasmic reticulum by SERCA (Sarcoplasmic reticulum calcium ATPase) and pumped out of the cell to a lesser extent by specialized calcium channels. Calcium ions dissociate from troponin C, and tropomyosin inhibition of actin-myosin interaction is restored.