Let’s go back to the 4th week during the development of heart. The primitive intraembryonic coelom forms in the lateral and cardiogenic mesoderm during 4th week of development.
Like the heart fields, the intraembryonic coelom has a horse-shoe configuration during this period:
- Anterior part: future pericaridal cavity (heart develops inside this cavity)
- Lateral parts: future pleuro-peritoneal cavities
A thick mesodermal plate called “septum transversum” lies cranial to the pericardial cavity during this period, before the folding of the embryo.
Folding of the embryo
The embryo undergoes 2 foldings during the 4th week:
- Lateral folding
- Cranio-caudal folding (due to the development of brain and enlargement of head-fold)
Due to the folding, coelom descends caudally below the developing brain:
- Pericardial cavity comes to lie ventrally
- The 2 limbs of Pleural cavity comes to lie dorsally and laterally
- Inferior venacava, Foregut and Aorta lies posterior to the pericardial cavity, between the 2 limbs of pleural cavity.
- Peritoneal cavity lies caudal to pericardial and pleural cavity
All these cavities are in communication with eachother.
Septum transversum:
- Septum transversum that lied cranial to the pericardial cavity also comes ventrally but lies caudal to the pericardial cavity.
- Septum transversum grows posteriorly but stops at the foregut, forming:
- Primitive diaphragm between pericardial cavity and periotneal cavity (divides pericardio-peritoneal canal)
- Peluro-periotneal canal are still in communication.
- Pericardio-peritoneal canal are still in communication.
Note: During this period, there is only one cavity – pericardioperitoneal cavity (pleuroperitoneal cavity doesn’t exist but the term has been use to make understanding easier). Pleuroperitoneal cavity is formed only when the lung bud develops from the ventral aspect of foregut at the level of septum transversum and grows to invade the pericardioperitoneal cavity.
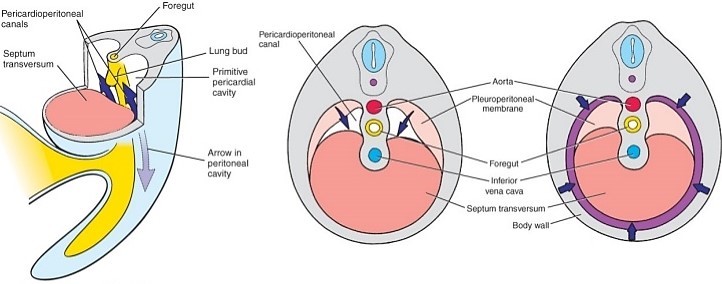
Pleuro-pericardial and Pleuro-peritoneal Membrane
By the end of 4th week, future pleural cavities are still in communication with the pericardial cavity and peritoneal cavity.
During 5th week, from the lateral wall of each pleuroperitoneal canal (more specifically pericardioperitoneal canal as discussed earlier):
- Cranial ridge grows as pleuopericardial fold and then as membrane
- Caudal ridge grows as pleuroperitoneal fold and then as membrane
Pleuropericardial membranes:
- Grow ventrally towards midline between the septum transversum and foregut.
- During 7th week: they fuse with eachother and with ventral mesentery of esophagus (foregut).
- Pleural and Pericaridal cavities are separate now.
- Right pleuropericardial opening closes before the left one, since the right common cardinal vein (future Inferior Venacave) is larger and produces a larger membrane.
Pleuroperitoneal membranes:
- Grow ventrally and medially towards septum transversum and dorsum of foregut.
- During 7th week: they fuse with each other and with septum transversum and dorsal mesentery of esophagus (foregut).
- Muscle fibers migrate from C3-C5 somite level to muscularize the membrane.
- Right pleuroperitoneal membrane also closes before the left one – reason is uncertain, but may be related to relatively larger size of the liver during this period.
Lateral Body Wall Covers Pleuro-peritoneal Membrane Externally
During 9th-12th week:
- There is progressive growth of lungs and the pleural cavities, “burrowing” into the lateral body walls.
- Tissue of body wall is split into 2 layers –
- External layer – forms definitive abdominal wall
- Internal layer – forms an additional rim around the pleuro-peritoneal membrane
- Derives innervation from lower intercostal nerves.
Descent of Diaphragm
At 4th week: Septum transversum lies opposite to C3-C5
- muscle cells for the diaphragm originate from somites at these segments, the phrenic nerve also arises from these segments of the spinal cord (C3, 4, and 5 keep the diaphragm alive!)
By 6th week: Diaphragm and phrenic nerve enters thoracic somite level.
By 8th week: Dorsal part of diaphragm lies at the level of L1.
Which structures derive which part of diaphragm ?
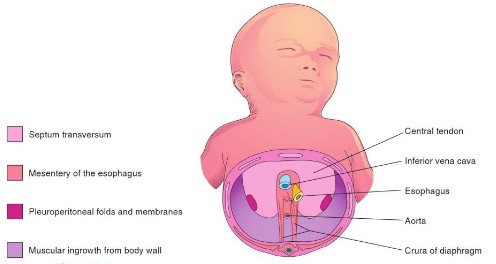
- Septum transversum: central tendon of the diaphragm
- Two pleuroperitoneal membranes: forms only a small part of the diaphragm
- Muscular components from somites at C3-C5: periphery of diaphragm
- Mesentery of esophagus: crura of the diaphragm
Timeline of Diaphragm Development or Embryology
- 4-5 weeks:
- Septum transversum grows and forms “pericardio-peritoneal” diaphragm
- Diaphragm descends from C3-C5 towards thorax.
- Phrenic nerve descends along with the diaphragm.
- 5-8 weeks: Pleuroperitoneal fold closes and forms “pleuro-peritoneal” diaphragm; Diaphragm descends to L1.
- 9-12 weeks:
- Lateral body wall mesenchyme forms additional rim around “pleuro-peritoneal” diaphragm.
- This peripheral rim derives innervation from lower intercostal nerves
Clinical Correlate
Congenital Diaphragmatic Hernia (CDH)
There are 3 types of CDH:
1. Posterolateral Bockdalek Hernia:
- Occurs through the vertebro-costal triangle (foramen of Bochdalek)
- Gap between vertebral and costal origins of diaphragm results from failure of closure of pleuroperitoneal canal (non-development of pleuroperitoneal membrane).
- More common on left side due to 2 reasons:
- As discussed earlier, right pleruoperitoneal canal closes earlier for unknown reason.
- Liver acts as buttress on the right side.
- Abdominal viscera may herniate into thoracic cavity and lead to pulmonary hypoplasia and respiratory distress soon after birth.
- Clinically, scaphoid abdomen in a neonate is typical of CDH.
2. Anterior (Retrosternal or Parasternal) Morgagni Hernia:
- Occurs through the sterno-costal triangle (foramen of Morgagni or Larry’s gaps)
- The sternal portion of diaphragm arises from the posterior rectus sheath and from the xiphoid process, and is not always present.
- A gap exists bilaterally between sternal and costal attachments.
- If hernia occurs, it is usually on the irght side.
3. Hiatal (Esophageal) Hernia:
- An abnormally large esophageal hiatus can allow the stomach to herniate into the pleural cavity.
- This incapacitates the physiological lower esophageal sphincter, allowing the contents of the stomach to reflux into the esophagus.
- This usually occurs in the adults.