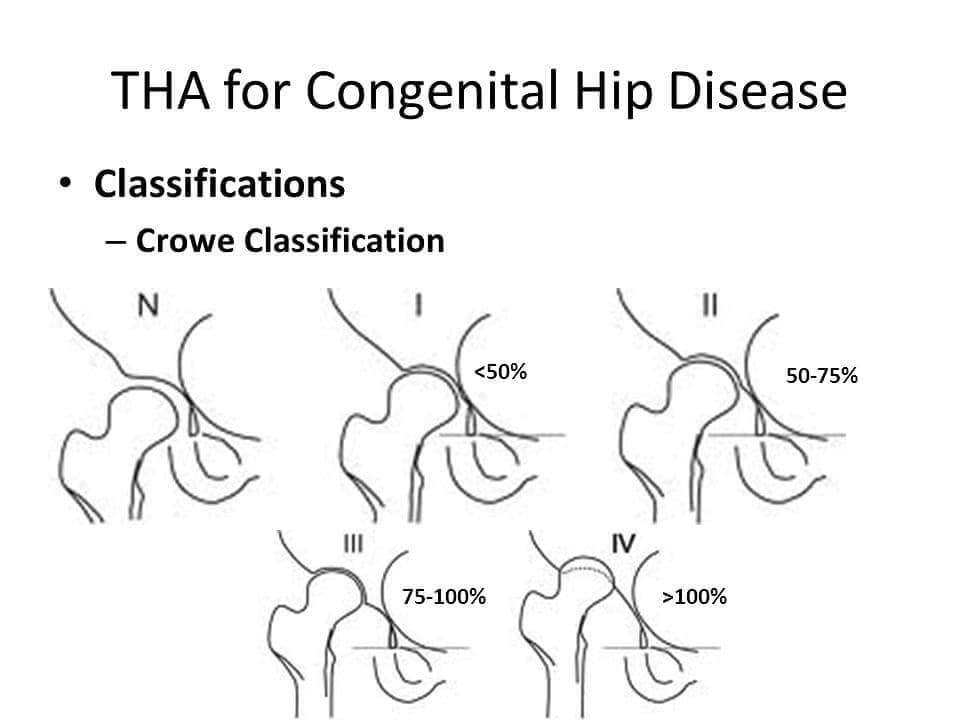
Crowe Classification
Crowe classification (1979) is based on 3 easily identifiable anatomic landmarks:
- Height of the pelvis
- Medial head–neck junction in the affected hip
- Inferior margin of the acetabulum (teardrop)
Reference line: drawn joining the inferior margins of each tear drop
Degree of dysplasia: distance from reference line to medial head–neck junction
The normal ratio of vertical diameter of the femoral head to the height of the pelvis is approximately 1:5. A hip is considered subluxated 50% or greater only if the medial head-neck junction was situated above the reference line by at least 10% of the measured height of the pelvis.
Class I: <50% subluxation of vertical diameter of femoral head or proximal displacement <10% of pelvic height
Class II: 50-75% subluxation of vertical diameter of femoral head or proximal displacement 10-15% of pelvic height
Class III: 75-100% subluxation of vertical diameter of femoral head or proximal displacement 15-20% of pelvic height
Class IV: >100% subluxation of vertical diameter of femoral head or proximal displacement >10% of pelvic height and deficient true acetabulum
Clinical Application
It aids to anticipate:
- Acetabular bone grafts
- Femoral shortening osteotomies
- Increased risk of neurovascular complications
| Crowe | Acetabulum | Femur | Approach |
| I | Uncemented component in true acetabular region with slight medialization | Cemented or uncemented stem based on patient age, bone quality, and bone geometry | Anterolateral or Posterolateral based on surgeon preference |
| II or III | Uncemented component at or near true acetabular region with autograft augmentation; or high hip center; or medialization | Cemented or uncemented stem based on patient age, bone quality, and bone geometry | Anterolateral, Posterolateral, Transtrochanteric, or Subtrochanteric approach based on reconstructive technique & need for femoral shortening |
| IV | Extra-small uncemented acetabular component in true acetabular region | Greater trochanteric osteotomy with sequential proximal shortening and cemented “DDH stem” or shortening subtrochanteric osteotomy and uncemented stem | Transtrochanteric or posterior approach with shortening subtrochanteric osteotomy |
Alternative classifications used
Hartofilakidis classification:
- Class A (Dysplasia): Head in acetabulum
- Class B (Low Dislocation): Head in false acetabulum which covers true acetabulum
- B1: False acetabulum covers >50% of true acetabulum (resembling dysplasia)
- B2: False acetabulum covers <50% of true acetabulum (resembling high dislocation)
- Class C (High Dislocation): Head superiorly migrated and not in contact with true acetabulum
- C1: Femoral head articulates with false acetabulum
- C2: Femoral head free floating within gluteal musculature