Definition of Brown Sequard Syndrome
Neurological syndrome resulting from spinal cord hemisection (damage to one lateral half of spinal cord).
Causes of Brown Sequard Syndrome
- Penetrating trauma
- Spinal fractures
- Spinal dislocation
- Disc herniation
- Vasculitis
- Radiation induced injury
Clinical Manifestations and Anatomical Basis of Brown Sequard Syndrome
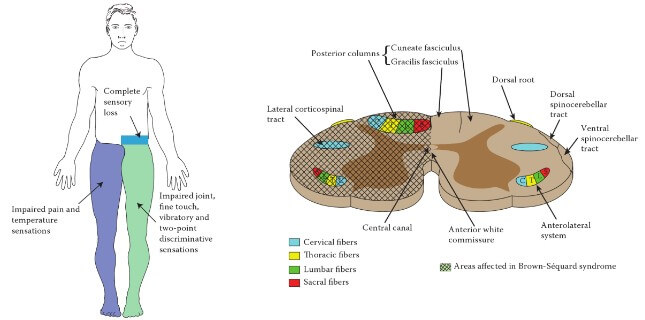
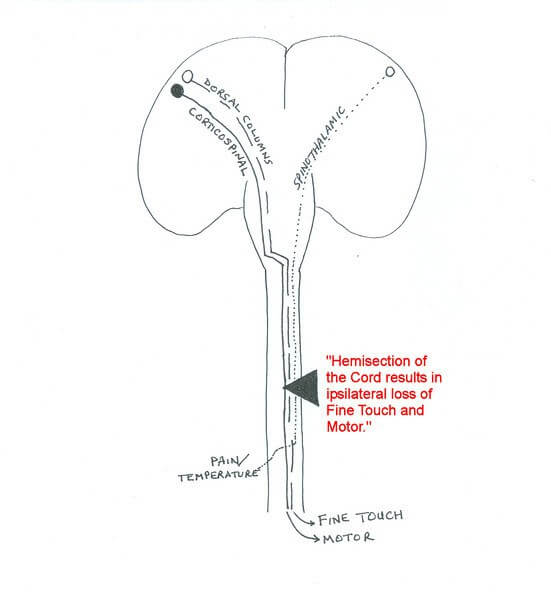
1. Damage of Corticospinal tract below the level of pyramidal decussation:
- Corticospinal tract crosses at the level of medulla – hence, the lesions below it will produce ipsilateral symptoms.
- Ipsilateral Upper Motor Neuron Lesions below the level of injury
2. Damage of Lower Motor Neurons at the level of Injury:
- Ipsilateral Lower Motor Neuron Lesions at the level of injury
3. Damage of Dorsal column below the level of sensory decussation:
- Dorsal column crosses at the level of medulla – hence, the lesions below it will produce ipsilateral symptoms.
- Ipsilateral loss of joint position sense, tactile discrimination, fine touch and vibratory sensations at and below the level of injury.
4. Damage of Spinothalamic tract:
- The fibers of spinothalamic tract ascend or descend 1-2 spinal segments in Lissauer’s tract to immediately cross and ascend in opposite side.
- Damage leads to contralateral loss of pain, temperature and crude touch sensation starting 1 or 2 segments below the level of lesion.
5. Destruction of posterior root and it’s entrance into spinal cord:
- Band of cutaneous anesthesia at the level of injury
6. Damage of Hypothalamospinal pathway:
- In lesions at and above T1 level.
- Ipsilateral Horner’s syndrome.
Bladder and bowel dysfunction may also be present in Brown-Sequard Syndrome (hemisection). But, its presence often indicates bilateral involvement of the spinal cord.
Dissociated Anesthesia
- Ipsilateral loss of Dorsal column sensations
- Contralateral loss of Spinothalamic tract sensations
Why doesn’t ataxia occur in Brown Sequard Syndrome ?
The ventral and dorsal spino-cerebellar tract also ascend laterally through the spinal cord. So, in the hemisection of the cord it is also supposed to be damaged resulting in ataxia. But you must be wondering that ataxia is not mentioned in most of the textbooks.
Ataxia does indeed occur in Brown-Sequard Syndrome but is typically masked by the weakness and hemiplegia resulting from damaged corticospinal tract. 1
Mnemonic: Bus STOP
Brown Sequard
Temperature Opposite Pain
Very nice explanation!!
I think the diagram may be wrong, as its showing contralateral loss of proprioception and ipsilateral pain loss.