The combination of excitatory and inhibitory signals in the basal ganglia circuit is pretty confusing. Let’s break the circuit and make them easy to understand.
There are 2 pathways in Basal ganglia circuit:
- Excitatory pathway
- Inhibitory pathway
Let’s declare 2 things first:
- Dopaminergic nigrostriatal projection increases motor activity.
- Cholinergic striatal projections decreases motor activity.
How does this happen ?
Both the Excitatory and Inhibitory Pathway Begin in Same Way
Excitatory input from the Cortex projects to the striatal neurons in the Caudate nucleus and Putamen.
Cortex —⊕→ Neostriatum (Caudate nucleus and Putamen)
Both the Excitatory and Inhibitory Pathway Ends in Same Way
1. Globus Pallidus interna projects inhibitory fibers to Ventrolateral Thalamus.
2. Ventro-lateral thalamus sends excitatory fibers to Motor cortex.
GPi —Θ→ VL Thalamus —⊕→ Motor cortex
Inhibit GPi to release inhibition from VL Thalamus to Promote Movement
This is what occurs in the Direct Pathway.
Cortex —⊕→ Neostriatum —Θ→ GPi —Θ→ VL Thalamus —⊕→ Motor cortex
- Inhibition of inhibitory fibers = Stimulation
- Simple mathematics: Minus X Minus = Plus
Stimulate GPi to inhibit VL Thalamus and Inhibit Movement
This is what occurs in the Indirect Pathway.
We need a intermediate pathway between the beginning and end of the common pathway to stimulate the Globus pallidus interna.
- Striatum projects inhibitory fibers to the Globus Pallidus externa (GPe).
- GPe projects inhibitory fibers to the Subthalamic nucleus (STN).
- STN projects excitatory fibers to the Globus Pallidus interna (GPi).
Cortex —⊕→ Neostriatum —Θ→ GPe —Θ→ STN —⊕→ GPi —Θ→ VL Thalamus —⊕→ Motor cortex
Again, the same equation:
- Minus X Minus = Plus (i.e. release of inhibition from subthalamic nucleus and excitation of GPi)
- Puls X Minus = Minus (i.e. stimulation of inhibitory GPi inhbitis thalamus and movement)
What did you notice till now ?
Direct pathway: Stimulates motor cortex
Indirect pathway: Inhibits motor cortex
Let’s come back to what we declared at the start
A. Dopamine facilitates movement:
2 Dopamine receptors in Putamen (Striatum): D1 and D2
Dopaminergic neurons projecting from Substantia nigra to Striatum:
- Act on D1 receptor —⊕→ Movement facilitating Direct pathway
- Act on D2 receptor —Θ→ Movement inhibiting Indirect pathway (i.e. facilitation of movement)
B. Acetylcholine inhibits movement:
- Cholinergic actions INHIBIT striatal cells of the Direct pathway and EXCITE striatal cells of the Indirect pathway.
- Thus the effects of ACh are OPPOSITE the effects of dopamine on the direct and indirect pathways so the ACh effects on motor activity are opposite those of dopamine.
Neurotransmitters in the Pathway
Excitatory = Glutamate
Inhibitory = GABA
Summary
The circuits do not cross i.e. they lie on the same side of the brain.
Direct pathway inhibits Globus Pallidus interna.
Indirect pathway stimulates Globus Pallidus interna.
Lesions of Basal Ganglia
Clinical signs in basal ganglia lesion are contrlateral to the side of lesion. This is because:
- Basal ganglia circuit doesn’t cross
- But, the corticospinal tract crosses to the contralateral side and Basal ganglia modulates the motor cortex.
A. Hypokinetic disorders – Lesions of Direct Pathway:
Parkinsonism Disease:
- Degeneration of Dopaminergic neurons of Substantia nigra and accumulation as Lewy bodies
- Inhibition of D1 receptor (Excitatory pathway) and Stimulation of D2 receptor (Inhibitory pathway)
- Also, ongoing unopposed ACh activity leading to activation of inhibitory pathway
- Inhibition of motor cortex and movement
- Accompanied by: TRAP
- Tremor (Resting pill-rolling)
- Rigidity (Lead-pipe and cog-wheel)
- Akinesia
- Posture (Stooped)
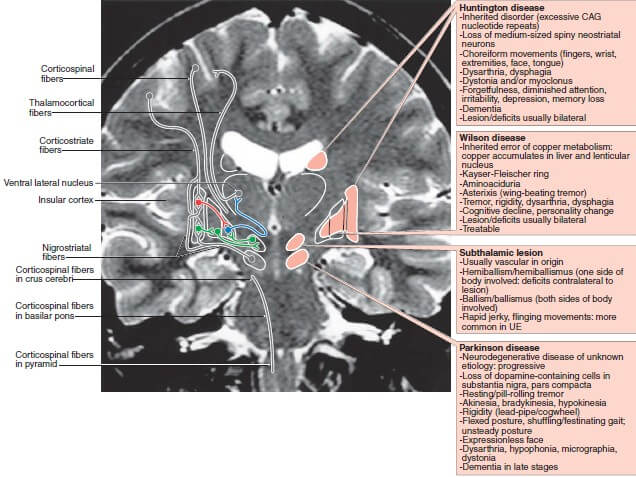
B. Hyperkinetic disorders – Lesions of Indirect Pathway:
1. Hemiballismus:
- Lesion of subthalamic nucleus
- No stimulation of GPi
- Violent projectile movement of limb seen contralateral to the lesion.
2. Chorea:
- Lesion of striatum (putamen)
- Initially, loss of GABAergic cells in the striatum that project only to GPe (inhibition of indirect pathway)
- Later, striatal cholinergic cells also begin to die
- Rapid, involuntary and purposeless jerks of irregular and variable location on the body
- Huntington’s chorea – due to excessive CAG (trinucelotide) repeats on chromosome 4
3. Athetosis:
- Lesion in the Globus pallidus
- Spontaneous and often continuous writhing movements of a hand, an arm, the neck, or the face.
4. Wilson’s Disease (Hepatolenticular degeneration):
- As the name suggests – lenticular dengeneration due to copper accumulation
- Lenticular or lentiform nucleus = Putamen + Globus pallidus
- Dystonia and Tremor are the most common hyperkinetic movement disorders in Wilson’s Disease.
5. Dystonia:
- Lesions in the lentiform nucleus (Putamen > Globus pallidus)
- Increased/sustained muscle contractions, twisting of the trunk or extremities, and abnormal postures.
The site of the lesions in various disorders is a subject of confusion as various sources have mentioned them differently. The lesion sites mentioned here are taken from the Textbook of Medical Physiology by Guyton and Hall.
C. UMNL vs LMNL vs Basal ganglia sings vs Cerebellar signs:
| LMNL | UMNL | Basal ganglia lesion | Cerebellar lesion | |
| Side of signs | Ipsilateral | Contralateral or Ipsilateral | Contralateral | Ipsilateral |
| Paralysis | Flaccid | Spastic | None | None |
| Muscle atrophy | Present | Absent (present if disuse) | None | None |
| Tone | Decreased | Increased | Increased | Decreased |
| Tendon Reflexes | Suppressed | Suppressed | Normal | Normal Or
Suppressed and pendular |
This is absolutely clear and helpful. Thanks so much.