Tricyclic Antidepressants (TCA)
Mnemonic: -pramine, -triptyline, -pin
- Secondary amines: predominantly norepinephrine reuptake inhibitors
- Nor-triptyline
- Desi-pramine
- Tertiary amines:
- Ami-triptyline
- Imi-pramine
- Clomi-pramine
- Doxe-pin
Irreversible MAO Inhibitors
Mnemonic: TIPS
- Non-selective MAO inhibitors:
- Tranylcypromine
- Isocarboxazid
- Phenelzine
- Selective MAO-B inhibitor:
- Selegiline (transdermal patch)
Reversible Inhibitor of MAO-A (RIMA)
- Moclobemide
- Tolaxatone
Tetracyclic Antidepressants
- Nonselective inhibitor of Serotonin and Noradrenaline like TCA:
- Amoxapine (also classified as secondary amine TCA) – also inhibits D2 receptor (also an antipsychotic)
- Maprotiline (also classified as secondary amine TCA)
- Noradrenergic and Specific Serotonin Antagonist (NaSSA): with central alpha-2 antagonistic activity resulting in release of NA and 5-HT
- Mirtazapine
- Mianserin
- Aptazapine
- Setiptiline
Selective Serotonin Reuptake Inhibitor (SSRI)
Mnemonic: flu-, par-, -pram and -traline
- Flu-oxetine
- Flu-voxamine
- Par-oxetine
- Ser-traline
- Citalo-pram
- Allosteric Serotonin Reuptake Inhibitor (ASRI): Escitalo-pram
Latency for antidepressant action:
Following reuptake or metabolism inhibition, NA and serotonin initially act on presynaptic alpha-2 and 5HT1A receptors respectively and decrease the firing of locus ceruleus (NA) and nucleus raphe magnus (5HT). On long term administration, desensitization of these receptors occurs and enhanced transmission is seen.
Noradrenaline and Dopamine Reuptake Inhibitor (NDRI)
- Bupropion (used for smoking cessation)
- Methylphenidate (used as stimulant in ADHD rather than depression)
Amphetamines are classified as NDRI or SNDRI (Serotonin, Noadrenaline and Dopamine reuptake inhibitors) – used in ADHD.
Noradrenaline Selective Reuptake Inhibitors (NSRI or NaRI)
- Reboxetine
- Atmoxetine (used in ADHD)
Serotonin and Noradrenaline Reuptake Inhibitors (SNRI)
- Venlafaxine
- Duloxetine
- Milnacipram
Functionally Serotonin and Noradrenaline Reuptake Inhibitors (SNRI):
- Tricyclic antidepressants (often referred to as “dirty” SNRI because they also possess anti-cholinergic, anti-alpha1 and anti-histaminic activity
- Tetracyclic antidepressants including NaSS
- SNRIs
Serotonin (5-HT2) Antagonist and Reuptake Inhibitors (SARI)
- Trazodone
- Nefazodone
Vortioxetine: serotonin reuptake inhibitor with 5HT3 antagonistic and 5HT1A receptor agonistic action.
Selective pre-synaptic 5HT1A partial agonist: Azapriones like Buspirone (anxiolytic)
Selective Serotonin Reuptake Enhancers (SSRE)
This action is opposite to that of SSRI.
- Tianeptine (Chemically TCA)
- Amineptine
Melatonergic antidepressant
- Agomelatine
Generation of antidepressants:
- 1st generation: TCAs, MAO inhibitors and RIMAs
- 3rd generation: Agomelatine
- 2nd generation: SSRIs and others
Antidepressants with Anxiolytic properties:
- SSRIs
- SNRIs
- TCAs
- NaSSAs
- MAO inhibitors
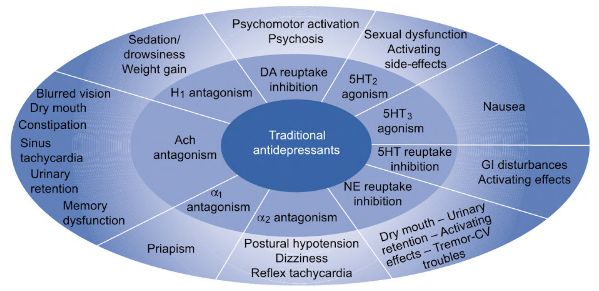
Adverse Effects of Antidepressants
Cheese reaction:
- Tyramine containing food (cheese, beer, red wine) + Non-selective MAO inhibitors = Tyramine escapes degradation = Hypertensive crisis
Serotonin syndrome:
- MAO inhibitor + SSRI (combination or within 2 weeks) = Increased serotonin
- When switching from one to another, “washout period” of 2-5 weeks is required.

Contraindicated Drug Combinations
- SRIs + MAO inhibitors
- Antidepressants + Sibutaramine
- SSRI + Nefazodone/Pimozide
- Serotonergic agents + Fenfluramine
Uses of Antidepressants
Mnemonic: DEPRESSION
1. Depression
1st choice of antidepressant: If there is a history of response to a specific drug or class, best 1st choice is that antidepressant.
SSRIs are often the primary choice because they are easy to use and have fewer side effects.
Mixed anxiety and depression: SSRIs, Other (Venlafaxine, Moclobemide)
- Avoid: Benzodiazepines
Atypical depression: SSRIs or Moclobemide (RIMA)
Melancholic depression: SNRI (Venlafaxine)
Psychotic depression: SNRI (Venlafaxine) or TCA with an atypical /antipsychotic
Underweight: Mirtazapine, Paroxetine or older TCAs
Increased sleep: Bupropion
Seasonal affective disorder: Phototheraphy, SSRI
Depression as a part of bipolar disorder: Mood stabilizer + SSRI or Buproprion (NDRI)
- Avoid: Monotherapy with antidepressant (risk of switch to mania or rapid cycling)
Cardiac problems: SSRI or other new non-TCA non-SNRI antidepressants
- Avoid: TCA, SNRI, MAO inhibitors
Asthma: Avoid MAO inhibitors (interaction with sympathomimetics)
Epilepsy: Older MAO inhibitors (only non-epileptogenic antidepressants)
- Bupropion cause seizures in patients with eating disorders
Glaucoma: Avoid TCAs (can precipitate acute narrow angle glaucoma in susceptible patients)
Obstructive uropathy: Avoid TCAs, MAO inhibitors and Trazodone (may retard bladder emptying)
Depression with OCD: SSRI, SNRI or Clomipramine
Depression with substance abuse: Cease or substantially reduce the amount consumed prior to commencement of antidepressant
Suicidal risk: SSRI and most new drugs
- Avoid: SNRIs and TCAs (considering lethality in overdose)
Children and adolescents:
- 1st choice: Psychosocial therapy
- Non-improvement and severe depression: SSRIs (Fluoxetine for <8 years)
Post-natal depression:
- 1st choice: Psychosocial therapy (from support to specific CBT)
- If on antidepressants before pregnancy: Continue the same antidepressant
- Severe depression, melancholia or suicidal risk: Antidepressants
- Sertraline or escitalopram are currently the most preferred SSRIs to use during pregnancy and breastfeeding.
- Fluoxetine is least preferred during breastfeeding because it has the highest infant serum levels.
- SSRI is associated with small risk of Persistent Pulmonary Hypertension in Newborn (PPHN).
- Paroxetine is associated with small risk of ventricular defects if taken in 1st trimester.
- Most antidepressants are classified as category C except:
- Category D: Paroxetine, Imipramine, Nortryptiline
- Category B: Maprotiline
2. Enuresis: Imipramine (TCA) but Drug of choice is Desmopressin
3. Premenstrual tension syndrome (PMS): SSRI
4. Phobia: SSRI
5. Recurrent panic attacks: SSRI
6. Eating disorders (Bulimia): SSRI
7. Stress disorder (PTSD): SSRI
8. Smoking cessation: Bupropion (NDRI)
9. Impulse disorder (Kleptomania): SSRI
10. Obsessive Compulsive Disorder (OCD): SSRI (Drug of choice), Clomipramine (Drug of 2nd choice)
11. Neuropathic pain
Approach to Depression Treatment in Short
Drug Facts
- Fluoxetine (active metabolite: norfluoxetine): prototype SSRI, longest acting drug
- Fluvoxamine: shortest acting SSRI
- Escitalopram: most specific SSRI
- Paroxetine: most teratogenic SSRI
- Most potent blocker of 5-HT reuptake: Paroxetine
- Least potent blocker of 5-HT reuptake: Bupropion
- Most potent blocker of NA reuptake: Desipramine
- Least potent blocker of NA reuptake: Mirtazapine
- Most selective inhibitor of 5-HT reuptake: Escitalopram
- Most selective inhibitor of DA reuptake: Bupropion
- Most selective inhibitor of NA reuptake: Oxaprotiline
- Maximum antimuscarinic activity: Amitriptyline
- Maximum antihistaminic activity: Nefazodone
- Maximum a1 blocking activity: Doxepin
- Minimum antimuscarinic, a1 blocking and antihistaminic activity: Venlafaxine
- Doxepin contains high antimuscarinic, antihistaminic and a-blocking (maximum) activities.
- Fluoxetine is longest acting and nefazodone is shortest acting antidepressant.
- Sertraline, citalopram. and escitalopram have the least interactions with other drugs and are sleep-wake neutral.
- Fluoxetine and Paroxetine are most activating drugs and should be taken in the morning.
- Fluoxamine is always sedating and should be taken in the evening.
- Onset of effect
- neurovegetative symptoms- 1-3 weeks
- emotional/cognitive: symptoms- 2-6 weeks
- How long to treat:
- 6-12 months: if 1st or 2nd episode
- 2 years: if third episode, elderly, psychotic featuras, refractory depression, > 2 episodes in 5 years
- Taper TCAs slowly (over weeks-months) because they can cause withdrawal reactions
- Tapering of any kind of antidepressant may be required based on the: half-life of the medication and the patient’s individual sensitivity
- It is important to be particularly vigilant over the first 2 weeks of therapy as neurovegetative symptoms may start to resolve while emotional and cognitive symptoms may not (patients may be particularly at risk for suicidal behaviour during this time)
- SSRI + TCA = Increased TCA concentration (due to CYP2D6 inhibition; most prominent with fluoxetine)
- TCAs are the only antidepressants in which effectiveness depends upon serum level. Nortriptyline is the only TCA with “therapeutic window”, i.e. at higher than therapeutic level – it not only increases risk of toxicity but also is ineffective.