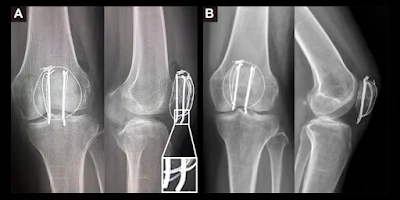
One month following an index TBW procedure (using 4 K‑wires + cerclage), our patient sustained a refracture of the patella after a fall. There was no high-energy direct trauma. This case typifies early failure of a classic TBW construct.
Failure Factors Identified in Literature
- Selçuk et al. (2025) found a 28% failure rate in TBW, with increased risk linked to single-knot cerclage, long K-wires (>69 mm), and lateral K‑wire placement >10.85 mm from articular surface
- Surgeons should aim for a K-wire length not exceeding 69 mm and a lateral K-wire to articular distance below 10.85 mm to minimize mechanical insufficiency.
Revision Fixation
- Employed tension-band wiring with cerclage augmentation, providing redundancy and rigidity
- The horizontal laceration overlapped with the previous incision; we extended it to reach the fracture site, preserving soft tissue integrity.
Alternate Techniques
- Double tension-band wiring with cerclage augmentation consistent with Xue et al.’s revision technique that yields 100% union rates and excellent function
- Insert 2 2.5-mm Kirschner (K)-wires distally from the proximal pole of the patella through the fracture site and the cortex of the distal fragment
- A stab incision is made at each end of the K-wires to expose the surface of the bone
- Two stainless steel wires is looped around the K-wires separately in a figure-eight manner.
- Tighten the loops to make them cling to the anterior surface of the patella and twist the steel wires at the insertions in the K-wires
- Cerclage wiring is then performed using a cable or a stainless steel wire
- For severely comminuted or lower‑pole fractures, non-absorbable braided suture with circumferential wiring can be an effective alternative achieving union in 14 weeks and minimizing metal hardware issues
Key Takeaways for Surgeons
- Early refracture (<6 weeks) often signals poor initial construct stability
- Critical technical factors include knot configuration, appropriate K‑wire length, and optimal wire placement relative to patellar anatomy
- A dual-band TBW with cerclage augmentation offers stronger fixation, especially in revision scenarios
- Alternate suture-based fixation can be useful in comminuted or soft-tissue compromised fractures

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.