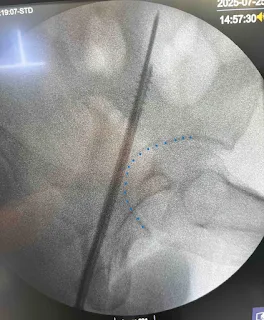
We operated on a 3-day-old left neck of femur (NOF) fracture in a 40-year-old male, performing a closed reduction and internal fixation (CRIF) with cannulated cancellous screws (CCS). The surgery was done without a fracture table, with the patient in supine position on a standard operating table. During intraoperative positioning for lateral imaging, loss of reduction occurred in 1-2 instances due to limb movement instead of adjusting the C-arm. Final fixation was done using three CCS in an inverted triangle configuration, although screws were not fully parallel. Today is going to be a bit of long post where I will be covering most of the important aspects of CCS fixation of femoral neck fractures.
Key Learnings
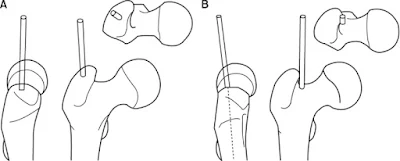
1. Garden type III vs Garden type IV neck of femur fractures
Garden’s III:
- Complete fracture with partial displacement
- Retinaculum of Weitbrecht remains attached to, & maintains continuity between, the proximal and distal fragments
- Trabecular pattern of femoral head does not line up with those of acetabulum, demonstrating incomplete displacement between femoral fragments
Garden’s IV:
- Complete fracture with total displacement
- No continuity between proximal and distal fragments
- Femoral head assumes its normal position within the acetabulum, and therefore the trabecular patterns of the acetabulum and the femoral head are aligned
Internal rotation traction radiographs constitute a simple, efficient and inexpensive tool to accurately determine both fracture line and displacement.
Gardens’ originally reviewed 80 patients with femoral neck fractures, which he classified in Types I to IV, and he followed these patients for at least 12 months postoperatively. He found that Types I and II fractures had a 100% union rate. Types III and IV had lower union rates of 93% and 57% respectively.
Displaced femoral neck fractures (Garden Types III and IV) are typically treated with internal fixation, hemiarthroplasty, or total hip arthroplasty (THA). Arthroplasty is preferred in older adults, while internal fixation is favored in younger patients to preserve the femoral head. Lu-Yao et al., in a meta-analysis found that internal fixation carries a high risk of nonunion (33%) and avascular necrosis (16%) in Garden’s III and IV fractures.
2. Indications of CCS in neck of femur fractures
- Physiologically young patient: age < 65, working patient, good bone stock
- Demented elderly patient that requires total care
- Adequate closed reduction with no fracture comminution or femoral neck defects
There are percutaneous and open techniques where fractures cannot be reduced by closed maneuvers.
Percutaneous technique of Su et.al., consists of the percutaneous insertion of two K-wires protecting the femoral artery by previous palpation, and the achievement of reduction and osteosynthesis by maneuvering the K-wires and inserting cannulated screws.
Mahajan et al. suggested another percutaneous reduction technique, which consists in the insertion of a K-wire to fix the femoral head to the acetabulum so as to mobilize the distal fragment in order to achieve anatomic reduction.
Two basic approaches have been described and applied for an open reduction: anterolateral approach by Watson Jones, and anterior approach by Smith-Petersen.
3. Garden’s alignment index and Lowell’s S line
Garden’s alignment index: It refers to the angle of the compression trabeculae on AP view relative to the longitudinal axis of the femoral shaft and the angle of compression trabeculae on the lateral view relative to the femoral shaft.
- AP view: angle should be 160 degrees
- Lateral: angle should be 180 degrees (collinear)
Acceptable reduction lies within range of 155-180 deg on both views which minimizes non-union and AVN.
When alignment index was < 155 degrees or > 180 degrees incidence of AVN rose from 7.3% to 53.8%.
Valgus reduction > 20 degrees results in increased rate of AVN.
Lowell’s S line: Follow the medial and the lateral cortical lines of femoral head and neck on the AP view and the anterior and posterior cortical lines on the axial view. Identify any translational and angular malalignment. The cortical lines should show intact Lowell’s S-patterns (“lazy S”) in both views.
4. Methods of closed reduction of neck of femur fracture
| Maneuver | Patient Position | Key Steps | Mechanism/Goal | Notes |
|---|---|---|---|---|
| Whitman | Supine, leg extended | 1. Apply longitudinal traction 2. Follow with abduction and internal rotation | Aligns femoral head via controlled rotation and traction | Simple technique; suitable for mild displacement (e.g. Garden III) |
| Wellmerling | Supine on fracture table | 1. Apply traction to equalize leg length 2. Add 1–2 cm of distraction 3. Use “wrestling hold”: forearms over (with elbow over groin) and under thigh 4. Apply internal rotation and elevate knee | Uses forearm leverage for controlled reduction in multiple planes | Technically demanding; avoid excessive force to preserve blood supply |
| Leadbetter | Supine, hip flexed to 90° | 1. Apply traction in line with femur 2. Internally rotate up to 45° 3. Slowly extend and abduct while maintaining rotation and traction 4. Assess with heel-palm test | Relaxes hip muscles and Y ligament; “opens book” to facilitate reduction | Preferred technique; useful in most displaced femoral neck fractures |
| Flynn | Supine, hip flexed 60–90° | 1. Apply traction and external rotation 2. Then apply internal rotation and extend the hip | Uses sequential rotation to reduce femoral head | Historical method; less commonly used today |
5. Fracture table vs Standard Operating table in CCS fixation
Doctors may choose to place the patient on a standard radiolucent table in a supine position, with a small pillow under the buttocks. This generally requires an assistant in order to keep the traction and manipulate the extremity during the surgical procedure and demands greater ability from the C-arm operator. Still, one of the benefits this table provides is that the whole extremity remains free, thus enabling an easier performance of closed reduction maneuvers.
The traction table offers the advantage of allowing the surgeon to control and keep the reduction, as well as facilitating visualization with the radiography equipment.
My experience reinforced that inadequate imaging strategy (moving limb instead of C-arm) may compromise reduction intraoperatively. Hence, to obtain the lateral view of the femoral neck in supine position in a standard operating table, the leg part of the operating table on the side of the healthy limb can be removed and the leg can be placed in the leg holder in a semi-lithotomy position with knee flexion of 90°, hip flexion of 90°, and hip abduction of 45°. A soft pad must be placed under the leg, which will be in the semi-lithotomy position, to reduce popliteal pressure.

6. Biomechanics of different CCS configuration in neck of femur fractures
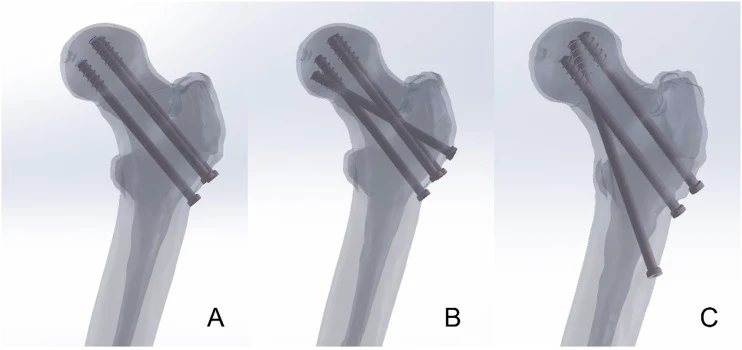
Three Cannulated Screws (TCS):
Inverted triangular, parallel configuration.
Screw positions:
- One inferior screw at the level of the lesser trochanter, close to the femoral calcar.
- Along or within 3 mm of the endosteum of the proximal aspect of the medial neck
- Two superior screws placed anteriorly and posteriorly near the femoral neck cortex.
- Optimally, the posterior cortex of the neck must be within 3 mm of the posterior wire to minimize the risk of retroversion collapse
Widely used due to low cost, minimal invasiveness, and preservation of blood supply.
Risks include excessive femoral neck shortening and lower stability, especially in unstable fractures.
Sequence of screw placement:
- First: Inferior (calcar) screw to resist varus collapse (inserted 1st and tightened at last to avoid varus axis deviation)
- Second: Posterior screw to resist retroversion of femoral head
- Last: Anterior screws
Further reading:
- Cannulated screws for Displaced subcapital femoral neck fractures
- Cannulated Screws for Femoral Neck Fracture : Wheeless’ Textbook of Orthopaedics
Four Cannulated Screws (FCS):
Adds a fourth “Pauwels” screw through the greater trochanter for enhanced anti-shear support.
Offers better overall stability and reduced risk of screw breakage in finite element modeling.
Biomechanically ideal for treating both stable and unstable FNFs
Biplane Double-Supported Screw Fixation (BDSF):
Screws placed in two oblique planes for multiplanar support.
Screw positions:
- Distal screw: Enters anterior one-third of the femoral shaft ~5 cm below trochanter, directed anterodistal to postero-proximal into dorsal femoral head.
- Middle screw: ~2 cm proximal to distal screw, angled postero-distal to antero-proximal into anterior femoral head.
- Proximal screw: ~1 cm proximal to middle screw, same plane and direction as middle screw.
Designed to resist shear forces, making it especially effective in Pauwels type III fractures.
Offers superior biomechanical stability in highly unstable fracture types.
Reference: Cui Z, Fan J, Cao Y, Fu Y, Bai L, Lv Y. Biomechanical Study of Three Cannulated Screws Configurations for Femur Neck Fracture: A Finite Element Analysis. Geriatr Orthop Surg Rehabil. 2024 Sep 16;15:21514593241284481. doi: 10.1177/21514593241284481. PMID: 39296708; PMCID: PMC11409286.
However, Sensoz et al. conducted a finite element analysis to evaluate entry point-related complications and showed that insertion of screws below the trochanter minor significantly increases the chance of a subtrochanteric fracture.
7. Timing of surgery
The ideal timing for surgical fixation of femoral neck fractures remains controversial. While traditional recommendations suggest performing surgery within 6 hours of trauma, evidence from multiple studies presents mixed conclusions:
Manninger et al. (1990s) found that surgeries within 6 hours had lower rates of nonunion and avascular necrosis (AVN) compared to those done after 6 or 24 hours.
Loizou et al. (2009), analyzing 1023 patients treated within <6 to 48 hours, found no significant difference in AVN incidence.
Upadhyay et al. compared outcomes before and after 48 hours and reported no significant difference in necrosis rates (overall 16.3%).
Papakostidis et al. (2015 meta-analysis) concluded that although earlier surgery is ideal, the exact time cutoff is unclear. Delays beyond 24 hours may be associated with increased risk of pseudoarthrosis, but stronger evidence is needed.
While early surgery is generally recommended, current evidence does not definitively link specific timing thresholds (e.g., <6 or <48 hours) with improved healing or lower AVN rates. However, delays beyond 24 hours may increase nonunion risk.
Further reading:1130-Texto del artículo-20056-1-10-20210211.pdf

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.