In orthopedic trauma surgery, complications often come unexpectedly which must be dealt critically. even routine procedures can throw a surprise. We came across one such unexpected complication while operating on a case of 23-year-old male with bilateral closed shaft of femur fracture with antegrade intramedullary interlocking (IMIL) nail on left side.
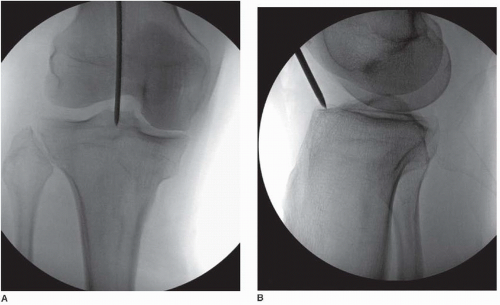
As we prepared to insert the proximal-most interlocking screw, the drill successfully crossed both cortices. However, just after purchasing the far cortex, the drill bit broke inside the bone.
How We Retrieved It
Instead of abandoning the screw or changing trajectory, we decided to retrieve the broken drill bit.
1. We extended the incision a bit anterior proximally
2. We manually palpated and located the tip of the broken drill bit at the far cortex
3. With the remaining shaft of broken drill bit, using a small hammer, we gently tapped the broken drill bit forward through the drill hole.
4. As the broken drill bit fragment became more prominent on the other side, we grasped it with the curved artery forceps.
5. Once, it was grasped, we gently tapped it out of the far cortex and pulled it out.
6. We completed the proximal screw insertion without need for redrilling or trajectory change.
- Always use sharp, undamaged drill bits
- Don’t force the drill—let it cut at its own pace
- Maintain accurate alignment of the drill sleeve/jig
- Replace old or overused drill bits promptly
How to prevent drill bit breakage:
1. Always use sharp, undamaged drill bits
2. Don’t force the drill – let it cut at its own pace
3. Maintain accurate alignment of the drill sleeve/jig
4. Replace old or overused drill bits promptly
I searched if there was any possible risk to neurovascular bundle during this procedure. This is what I found:
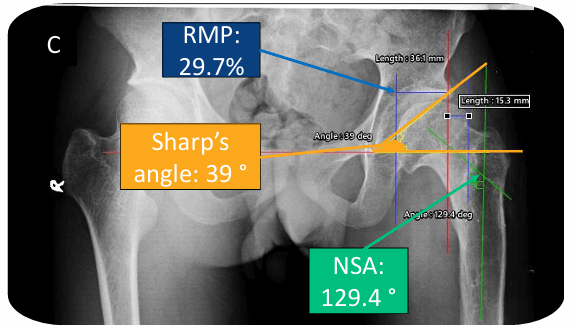
The neurovascular bundle, consisting of the femoral nerve, artery, and vein, is situated more anterior and lateral to the lesser trochanter, closer to the femoral neck and shaft. While the iliopsoas muscle and its tendon lie adjacent to the neurovascular bundle, they are more closely associated with the lesser trochanter than the neurovascular structures themselves.
Further reading and other techniques:
- “Push back” technique: A simple method to remove broken drill bit from the proximal femur – PMC
- Removal of Broken Drill Bits and Locking Screws from an Intramedullary Nail – PMC
We also faced difficulty while reaming through the proximal femur as it encountered the thick lateral cortex. This might have happened due to an incorrect entry point. Lets discuss the entry points for antegrade IMIL nailing of femoral shaft.
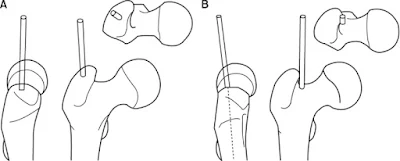
a. Trochanteric entry point:
- Used for proximally curved nails (has valgus bend proximally to accommodate GT)
- Just lateral to the tip of the greater trochanter in the AP view
- Exactly centered on the axial view, in order to prevent eccentric reaming
b. Piriformis entry point:
- Used for straight nails
- Just medial to the tip of the greater trochanter.
- In certain cases, the greater trochanter may be curved and medialized. It may then be necessary to ream through the medial tip of the greater trochanter.
- Main advantage is a colinear trajectory with the long axis of the femoral shaft
- Anterior bow of shaft curves up to posterior tip of greater trochanter (hence, beginning awl should be inserted just posterior to midline of trochanter and just medial to prominence of trochanter in trochanteric fossa)
- When an IM guide wire is passed in retrograde manner in cadaver femora, entry point is slightly anterior in piriformis fossa. However, entrance portal anterior to the midpoint of the trochanter may result in perforation of the anterior cortex of the proximal femur.
- Entry that is too far anterior results in deformation of nail & comminution of the proximal fragment
- Entry that is too far medial, may result in femoral neck fracture
- For nails that are designed for piriformis entry, lateral placement through the trochanter may cause varus alignment of proximal fractures

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.