Today’s case involved a 63-year-old female presenting with a right iliac wing fracture (Tile A2) and a left distal radius fracture following trauma. The pelvic injury was managed with open reduction and internal fixation using reconstruction plates and a screw via the lateral window of the anterior approach. The distal radius fracture underwent closed reduction and percutaneous pinning in the same surgical session. This article discusses the Tile classification, surgical exposure through the lateral window, and fixation principles for iliac wing fractures.


Tile classification – Where does this case fit?
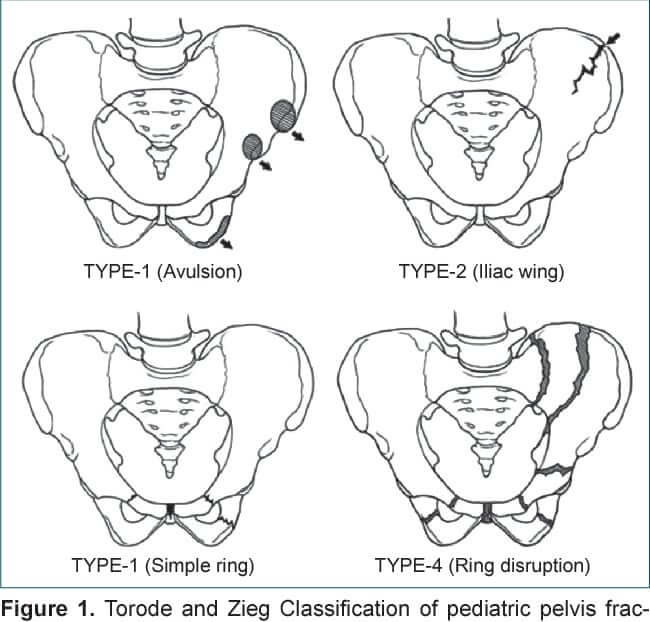
The Tile classification is one of the most widely used systems for pelvic ring injuries, focusing on stability based on the integrity of the posterior sacroiliac complex.
Read the details of Tile Classification here: Pelvic Fracture Classification and Management : Simplified | Epomedicine
Tile A2: Stable fracture of the pelvic ring without posterior arch involvement, e.g., isolated iliac wing fracture.
Mechanism often: Direct blow or low-energy lateral compression.
Lateral window of ilioinguinal approach
The anterolateral Olerud approach, corresponding to the first window of the ilioinguinal Letournel approach, allows exposure of the iliac wing and direct access to the anterior part of the SI joint.
Three windows are developed to allow visualization of the pelvis and acetabulum:
- Lateral – between the iliac wing and the iliopsoas muscle
- Middle – between the femoral nerve (iliopsoas muscle) and the external iliac vessels
- Medial – between the lymphatics and the rectus abdominus at the level of the pubic tubercle
This lateral window approach is used for reduction and fixation of:
- Iliac wing fractures
- Transiliosacral “crescent” fractures
- Disruptions of the SI joint
Sacral fractures cannot be adequately exposed and fixed through this approach.
Positioning:
- Supine
- Foley necessary
- Flat top radiolucent table or traction table
- Lumbosacral bump
- Leg can be prepped out or in
- Hip flexion to relax iliopsoas – Towel bump, bone foam ramp, or table
- Prep to chest cranially and buttock posteriorly
Incision:
- An incision is made along the iliac crest. Be aware of the lateral femoral cutaneous nerve in the region of the ASIS. The length of the incision is determined by the amount of area that needs to be accessed in the iliac fossa.
- The incision can be extended intraoperatively depending on the necessary exposure.
- For fractures involving the posterior aspect of the ilium, or the SI joint, the exposure needs to be extended posteriorly almost to the table.
Superficial dissection:
- Divide the subcutaneous tissues in line with the skin incision in order to expose the fascia overlying the external oblique muscle.
- Identify the border between the gluteus muscles and external oblique muscles. Incise the muscular interval with electrocautery.
- The external oblique muscle is subperiosteally elevated from the iliac crest. At this time, the lateral cutaneous femoral nerve, which runs ventrally to the anterior superior iliac crest, has to be spared.
- With a small elevator, the iliac muscles are elevated using the same subperiosteal layer.
Deep dissection:
- When elevating the iliacus muscle, bleeding from nutrient vessels can occur and should be stopped with bone wax.
- Continue with careful blunt dissection to the interior part of the SI joint medially to the pelvic ring.
- Proceed anteromedially at the pelvic rim as far as to where the iliopectineal eminence begins.
- Continue the dissection with an instrument such as a Cobb elevator.
- The SI joint capsule should be identified. Place a Hohmann retractor into the superior portion of the SI joint.
Expose the SI joint (if needed):
- The dissection is carried further medially as far as the sacral ala, which visualizes the upper part of the anterior column. Move the Hohmann retractor medially carefully onto the sacral ala.
- Note the L5 nerve root traversing this region.
- Place a second Hohmann retractor more anteriorly on the sacral ala if required.
- Place an additional Hohmann anterior to the SI joint for additional exposure. Take care when placing this anterior retractor as it may injure the superior gluteal artery and nerve as they exit the greater sciatic notch.
- The anterior column as far as the SI joint is now exposed.
Further reading:Anterior intrapelvic approach to the acetabulum
Reduction techniques for Iliac wing fractures
Closed reduction techniques:
Schanz screw (can be used as joysticks)
Open reduction techniques:
- A clamp (e.g. Farabeuf) may be used to grasp the iliac crest to manipulate and reduce the fragment.
- A ball spike pusher may also be used to aid in reduction. The ball spike may be placed along the pelvic brim or alternatively, the ball spike may be placed at the anterior inferior iliac spine directed posteriorly.
- A Schanz screw (joystick) may be inserted into a fragment of the iliac wing for reduction of the fracture fragment.
- Another method to aid in reduction is to use a pointed reduction clamp at the iliac crest to manipulate and reduce the fracture fragment.
- Alternatively, screws may be placed into the fracture fragments and grasped using either a Farabeuf or a Jungbluth clamp to achieve reduction.
Verification of reduction:
- Closed reduction: Fluoroscopy in multiple planes
- Open reduction: Fluoroscopy + Palpation (along ilium and at pelvic brim)
Fixation of Iliac wing fractures
After reduction is achieved, the fracture may be stabilized with plates and/or interfragmentary lag screws.
Contoured recon. plates:
- The best bone for fixation is along the iliac crest and adjacent to the pelvic brim. Between these regions, the bone is thin and it is difficult to achieve satisfactory fixation.
- After reduction, a contoured reconstruction plate may be placed along the iliac crest.
- The plate may be placed on the inner surface of the ilium spanning the fracture lines with ideally two screws on each side of the fracture. Alternatively, a plate may be applied directly to the superior surface of iliac crest.
- A plate may also be applied across the fracture, in compression mode, at the level of the pelvic brim.
Intramedullary screws:
- Fracture lines that extend to the iliac crest may be stabilized with 3.5 mm interfragmentary lag screws.
- These screws are placed in an intramedullary fashion between the inner and outer table of the ilium.
- Another method of fixation is a long intramedullary lag screw that is placed from the anterior inferior iliac spine extending to the posterior ilium. This is typically a 6.5 mm or 7.3 mm partially threaded cannulated screw.

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.