Components of pronator drift
Progress from distal to proximal:
- Downward arm drift
- Forearm pronation
- Flexion of the wrist and elbow
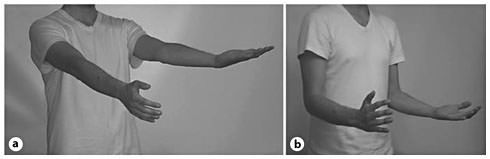
Method of assessment for pronator drift
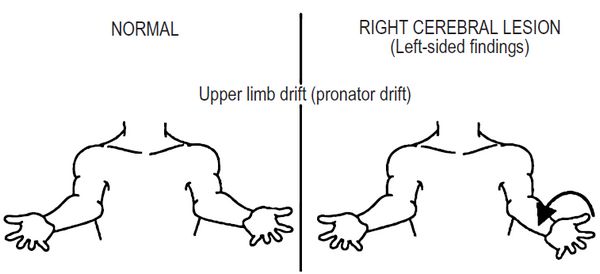
When the patient extends both arms upright in the supinated position and hold them at shoulder height for atleast 10 seconds (Patients should be asked to keep eyes open initially and later test again with eyes closed):
- Normal response:
- Palm will remain flat, elbows straight and the limbs horizontal OR
- Symmetrical deviation from this position (i.e. on both the sides – dominant hand may pronate slightly more than the non-dominant hand)
- Positive pronator drift:
- Components of pronator drift as mentioned above is seen in the weaker side (asymmetric response) which indicates a lesion in contralateral
- Pseduodrift:
- Slight pronation, without downward drift of the dominant arm
- Not necessarily abnormal – must be interpreted in clinical context
The examiner can simple wait for the response or hasten the process by tapping on the patient’s palms or having the patient turn the head back and forth, or both.
Interpretation of positive pronator drift
- Positive with eyes open: Motor deficit
- Positive with eyes closed: Sensory deficit (Posterior column)
- Outward and upward drift: Cerebellar drift
- “Updrift” (involved arm rising overhead without patient awareness): Parietal lobe lesions (loss of position sense)
- Drift without pronation: Functional upper limb paresis (Conversion disorder)
Importance of Pronator Drift
- Can detect subtle upper motor neuron lesion which goes unrecognized by routine motor examination
- Included in the initial examination of stroke as “FAST”
- If only one motor test could be done in a patient – the best single test would be to examine the drift
Mechanism of Pronator Drift
Here, we will try to answer the questions like:
- Why pronator drift occurs when eyes are closed?
- Why pronator overcomes supinator in pyramidal lesion?
According to Phylogenetic theory of Gierlich:
- Similar reflex was seen in newborns with pyramidal system not fully developed – confirmation that this sign was related to dysfunction of the pyramidal tract
- Pronation, associated with flexion and abduction movements, represents the most important movement in amphibians, fish and reptiles – necessary to set the water back and to move forward, and that it is still strongly present in mammals.
- A complete supination is possible only among the most evolved animals, so that the palm of the hand can be completely turned upwards; the second part of the outward rotation movement appears then to be related to the formation and development of the pyramidal pathways.
Thus, the pronation dependent upon phylogenetically older subcortical centers overpower those dependent upon phylogenetically newer pyramidal system when impaired. Moreover, some neurologists have proposed that, phylogenetically younger structures like pyramidal tract have more propensity to be affected by pathological processes compared to older structures.
Other authors have proposed that:
- Cortico-spinal tract (CST) muscles in the upper extremity are the extensors, supinators and abductors
- These CST muscles are minimally weak in subtle CST lesions
- Hence, the uninvolved and stronger non-CST muscles overcome the minimally weakened CST muscles – elbow flexes, hand pronates and the arm drifts downwards
- If the whole area of cortex supplying a limb is damaged, the extrapyramidal pathways are unable to take over and an acute global flaccid paralysis of the limb occurs
When visual cues are removed, subtle UMN weakness causes the weak limb to drift downward.

thanks for a wonderful explanation.
The test can be done in a confident and logical manner ,now that the explanation is there
Excellent!! Thank you!
Hello,
Thank you for making this available, it is very informative and for medical information, fairly easy to follow. My three-year-old son has cerebral palsy, specifically diagnosed with spastic diplegia. He does not seem to be able to turn his hands Palm up, does this suggest that he is possibly mild quad?
Hello Amber,
Diplegic cerebral palsy is the commonest anatomical type of cerebral palsy. In diplegia motor abnormalities is seen in all four extremities with lower extremities more affected than the upper. Spasticity of the pronator muscle can lead palm facing towards floor and an inability to turn the palm up.
Finally, an excellent and thorough explanation I can apply in practice. Thank you.