Peculiarities of cerebral circulation:
1. Brain and spinal cord is isolated from endothelium by BBB composed of continuous capillaries that limits movement of proteins and electrolytes
2. Fluid movement is primarily determined by osmolar gradient (in contrast to peripheral tissues – transcapillary gradient of large macromolecules)
3. Hence, administration of large volumes of iso-osmolar crystalloid will result in peripheral edema owing to dilutional reduction of plasma protein content, but does not generally increase brain water content or intracranial pressure (ICP).
4. Hyperosmolar solution – decrease ICP; Hypo-osmolar solution – increase ICP
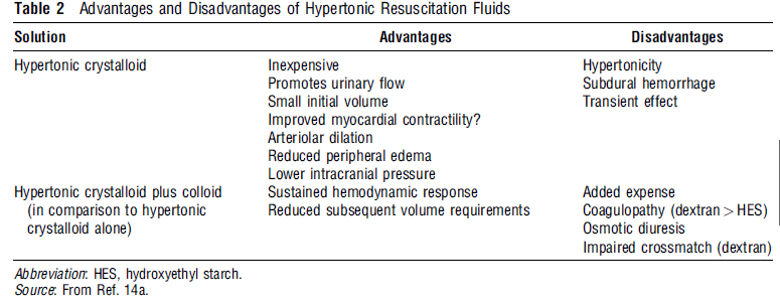
Choice of fluids in head trauma:
In one study, Hetastarch have been found to be beneficial over hypo-osmolar or iso-osmolar iv fluids: One possible explanation is that Traumatic Brain Injury (TBI) modifies the permeability of the BBB so that small solutes can pass easily while proteins pass less readily, i.e., after TBI the BBB may behave similarly to the systemic circulation.
In localized brain lesion with disruption of BBB, hypertonic fluids was beneficial in decreasing ICP – The most likely mechanism for the reduced ICP is a decrease in brain water content in regions remote from the lesion i.e. Edema of injured brain is compensated by dehydration of normal brain
1. Head trauma with hypotension: Isotonic crystalloid solutions (preferably 0.9% saline) are often the first solutions
2. Head trauma with raised ICP: Mannitol 20% (0.5 g/kg) followed by 0.25 g/kg 6 hrly may be appropriate (may cause hypotension in patient with occult hemorrhage)
3. Head trauma with raised ICP and Hypotension: Hypertonic solutions
4. Hypovolemia is best avoided in head injury – increased risk of secondary brain injury and mortality