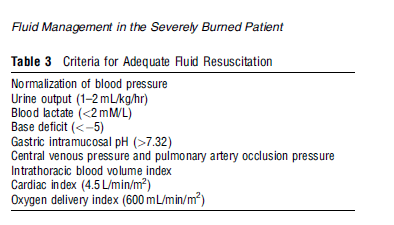
A) Clinical endpoints suggesting adequacy of burn fluid resuscitation:
- Increased vascular permeability
- Decreased intravascular volume and Edema
- Hypotension due to hypovolemia and myocardial dysfunction
- Compensatory rise in systemic vascular resistance
- Hyperdynamic circulation (SIRS) in 3-4 days postburn state if patient survives initial burn state and is resuscitated adequately
C) Goal of fluid resuscitation in burn: to sustain tissue perfusion while minimizing interstitial edema
D) Indication of fluid resuscitation in burn: partial thickness or full thickness burn involving 10-15% BSA
E) Principles of fluid resuscitation in burn:
- Minimal fluid to maintain organ perfusion
- Continuous titration
- Over-resuscitation can exacerbate burn edema and cause compartment syndrome
F) Burn fluid calculation:
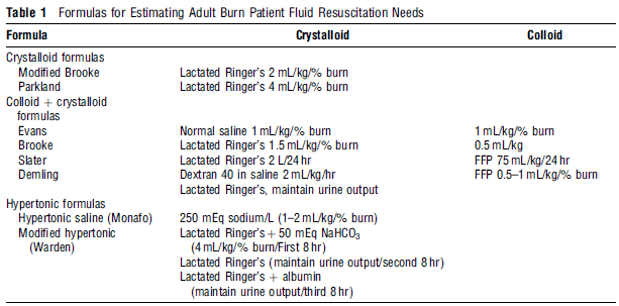
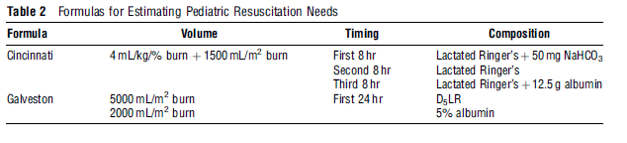
Burned children require usual maintenance fluids in addition to the volume that is predicted by the Parkland formula. In addition, albumin is commonly added to the resuscitation fluid due to the rapid fall in serum albumin levels that are commonly observed in children.
Practice – The Consensus formula:
A. The Formula: 2–4 mL lactated Ringer’s × body weight (Kg) × %TBSA burns = total fluid for the first 24 hr.
B. For the first 8 hours after injury, give half the total calculation.
C. Second and third 8 hr after injury, give one-fourth the total calculation.
Edema formation is most rapid during the first hours after injury, but continues for at least 24 hr. Therefore, half the calculated fluid is given in the first 8 hr following the burn.
Formulas only tell you where to BEGIN resuscitation, which must then be guided by patient response: urine output, vital signs, and mental status.
Example:
A 100 kg man is burned over all of both legs, his chest, and both arms. Calculated burn size is 65% TBSA.
Calculated fluid requirements: The Consensus formula offers a range of options, from 2 to 4 mL/Kg/%TBSA.
Therefore, calculations range between the following:
Minimum: 2 mL × 100 kg × 65%TBSA = 13,000 mL in 24 hr
= 6,500 in first 8 hr = 812 mL/hr
= 3,250 mL in each of the second and third 8 hr = 406 mL/hr
Maximum: 4 mL × 100 kg × 65% TBSA = 26,000 mL in 24 hr
= 13,000 mL in first 8 hr = 1,625 mL/hr
= 6,500 mL in each of the second and third 8 hr = 812 mL/hr
Adjust according to patient response
- You select an initial rate of 812 mL/hr, based on a calculation of 2 mL/kg/%TBSA. After 6 hr, the patient has received 4,872 mL of lactated Ringers. Urine output, which was initially good, has fallen to 20 mL in the past hour. Heart rate is 132, BP is 106/50.
- At this point you should increase the fluid rate, typically by about 10%–20%. All indications point to inadequate resuscitation.
- You increase fluids by 20%, to 974 mL/hr. Two hours later urine output again drops, to 15 mL/hr. Heart rate is 128, BP is 98/52.
- You should again increase fluids. Most experts would NOT consider use of a diuretic at this point in time. Individual fluid requirements vary significantly, and this man appears to need more than the minimum requirements. Even if you had selected an initial rate of 1,625 mL/hr, your response to decreasing urine output should be the same—to increase fluids.
- Three hours later, urine output has increased to 95 mL/hr. Heart rate has dropped to 90, BP is 135/85.
- You should now begin to decrease fluids by 10%–15% per hour, with continued attention to urine output and vital signs. Fluid resuscitation is a dynamic process and requires continuous attention to detail.
G) CHOICE OF FLUIDS IN BURN RESUSCITATION:
- Resuscitation should consist primarily of isotonic crystalloid solution because it is inexpensive, readily available, and can be given in large quantities without harmful side effects.
- Because injured capillaries are porous to proteins for the first several hours after injury, colloid-containing fluids are not used initially. Use of colloid in 1st 8-24 hours may worsen edema (increased vascular permeability)
- Use of hypertonic saline may be beneficial in battlefield conditions or if at increased risk of CHF but may cause hypernatremia.
- Glucose solution is contraindicated in 1st 24 hours: Hyperglycemia because of stress response
- Fluid to be used 24 hour postburn: Colloid; use D5W and 5% albumin at 0.5 ml/kg/% burn surface area
- Need of free water: Massive sodium load of RL in 1st 24 hrs and massive water evaporation
- Capillaries begin to work
- Water evaporation is highest from third degree burns
Sources and References: 1. Perioperative fluid therapy - Hahn 2. General Principles of Surgery - Peter F. Lawrence