Before beginning the clinical approach to a child with edema, it is necessary to understand the basics of fluid compartments, starling forces and technique of eliciting edema.
Life threatening causes of Edema:
Generalized:
- Cardiac disease
- Congestive Heart Failure
- Pericardial effusion
- Renal disease
- Nephrosis
- Nephritis
- Hepatic failure
Localized:
- Allergic reaction with airway involvement
- ACE inhibitor induced angioedema
- Cellulitis
- Group A Streptococcus with Varicella
- Snake bite
- Thrombophlebitis
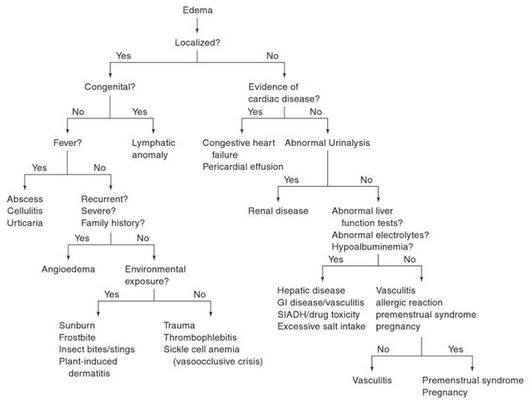
APPROACH TO LOCALIZED EDEMA:
1. Common causes:
| Fever | Local tenderness | Local warmth | Lesion/color | |
| Allergic reaction | No | No | Yes | Erythematous |
| Trauma | No | Yes | No | Violaceous |
| Infection | Usually | Yes | Yes | Erythematous or Violaceous |
A therapeutic response to an oral antihistamine or an intramuscular dose of epinephrine can help to differentiate an allergic reaction from other causes.
2. Other Aids to Diagnosis:
- Bilateral upper eyelid edema: Infectious mononucleosis (Hoagland’s sign)
- Severe or recurrent facial edema with positive family history: Hereditary angioedema
- Acute facial edema with cyanosis or plethora: SVC obstruction
- Other causes of facial edema: Oral, dental or sinus infections
- History of environmental exposure: Sunburn, frost-bite, plant-induced dermatitis
- Infant with unexplained localized swelling of extremity since birth:
- Birth trauma
- Congenital lymphedema (Milroy’s disease)
- Turner’s syndrome (Bilateral limb edema)
- Noonan’s syndrome (Pedal edema)
- Swollen and painful digits (dactylitis): Sickle cell anemia
- Weightlifting, OCPs: Thrombophlebitis or DVT
APPROACH TO GENERALIZED EDEMA
A. History:
| Components | Significance |
| Age of onset | Newbornvs Older children |
| Mode of onset | Sudden (<72 hrs)- Acute Nephritis, Allergic reaction |
| Site and evolution | Legs → Face → Ascites (Cardiac)Ascites → Legs → Face (Hepatic)
Face → Legs → Ascites (Renal) |
| Timing | Increase in morning – HypoproteinemiaIncrease in evening – Congestive cardiac failure |
| Exposure | Medications,Danders, Food preservatives – Allergic reaction |
| Nutritional history | Low protein intake – PEM |
| Past/Allergic history | Sore throat and joint pain – Rheumatic carditis Neonatal umbilical vein sepsis or Umbilical vein catheterization – Hepatic cause Chronic illnesses, Persistent diarrhea – PEMMilk allergy, Gluten sensitivity – Protein losingenteropathy |
| Associated symptoms | Significance |
| Orthopena, PND, Noisy breathing, Poor weight gain, Feeding difficulties, Bluish episodes | Cardiac cause |
| Yellowish discoloration, Dark urine, Black tarry stool, Pain/lump in abdomen, Itching, Petechiae | Hepatic cause |
| Rashes, joint pain | Connective tissue disorders |
| Nausea, vomiting, retarded growth | Uremia |
| Frothy urine | Nephrotic syndrome |
| Blood in urine, decreased urine | Nephritic syndrome |
| Anorexia, lethargy, diarrhea, vomiting, decreased growth, frequent infections, night blindness | Malnutrition |
| Cow milk intake, foul diarrhea, recurrent abdominal pain, frequent infections | Protein losing enteropathy |
B. General Physical Examination
| Findings | Significance |
| Tachycardia, Prolonged CRT | Cardiac diseases |
| Hypertension | Acute Nephritic Syndrome |
| Tachypnea | Pulmonary edema |
| Raised JVP | Congestive cardiac failure |
| Altered consciousness Disoriented |
Hepatic Encephalopathy Hypertensive Encephalopathy (Renal) |
| Asterixis | Hepatic encephalopathy |
| Pallor | Anemia, Malnutrition |
| Icterus, spider angioma, other stigmata | Chronic Hepatic diseases |
| Cyanosis and clubbing | Congenital Heart Disease |
| Flag sign, Bitot’s spot, Stomatitis, Muscle wasting, Dehydration, Hypothermia | Malnutrition |
| Abnormal anthropometry | Malnutrition |
C. Systemic Examination – Diagnostic Aids
- Gallop, Tachycardia, Tachypnea, Inspiratory crackles or Hepatomegaly: Cardiac disease
- Pericardial rub, Pulsusparadoxus, Muffled heart sounds, Jugular venous distension: Pericardial effusion
- Hepatosplenomegaly and Ascites: Hepatic cause (If no icterus – exclude portal vein thrombosis)
- Hepatomegaly (fatty liver): Malnutrition
GENERAL INVESTIGATIONS
- Urine dipstick and microscopy:
- Proteinuria, casts and hematuria are indicative of renal disease
- Renal function test and electrolytes:
- Raised serum urea and creatinine are indicative of renal disease
- Hyperkalemia, Hypokalemia, Hyperphosphatemia, Hypocalcemia
- Full Blood Count and Peripheral Blood Smear
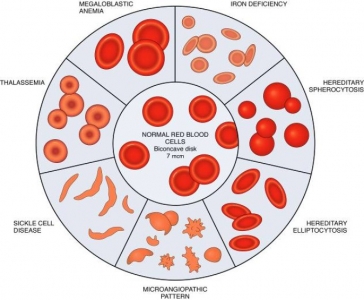
- normochromic normocytic anaemia suggest chronic disease
- hypochromic microcytic anaemia suggest iron deficiency from occult gastrointestinal bleeding i.e. cows milk allergy
- megaloblastic anaemia suggest vitamin B12 and folate deficiency from small bowel disease
- eosinophilia suggest angioedema or protein losing enteropathy
- Liver function test (LFT)
- Hypoalbuminaemia in the absence of circulatory overload suggests hypoproteinaemic states
- Hyperbilirubinaemia and transaminitis suggest liver disease
- Chest X-ray and electrocardiogram
- Cardiomegaly with prominent perihilar vascular marking and left ventricular hypertrophy confirms intravascular fluid overload
- ST elevation with t wave inversion (Pericarditis)
- ECG can provide clue to other causes of heart failure
SPECIFIC INVESTIGATIONS
Depending upon the most likely cause
- Cardiac cause: Echocardiography
- Nephrotic syndrome: 24 hour urine protein, Urine protein to creatinine ration, Fasting lipids, Screen for secondary causes e.g. SLE, Hepatitis B
- Nephritic syndrome: Serum complements, Screen for secondary causes e.g. Streptococcal infection, SLE, IgA nephropathy
- Chronic Liver Disease: Screen for underlying cause, Assess complication e.g. Hyperammonemia, Coagulopathy
- Cow’s milk allergy: FAST test for cow milk IgE, Patch test, Jejunal biopsy
- Gluten hypersensitivity: Anti-gliadinIgG/IgA, Anti-endomysialIgA, Jejunal biopsy
- Malnutirtion: Blood glucose, Septic screening, Stool & urine for parasites & germs, Electrolytes, Ca, Ph & ALP, serum proteins, CXR & Mantoux test, Exclude HIV & malabsorption
PRINCIPLE OF TREATMENT
- First principle: Reversing the primary disease
- Second principle: Restore hemodynamics and cardiac output
TREATMENT OF LOCALIZED EDEMA
- Insect bite reaction:
- Anti-histamine
- Anti-inflammatory (topical corticosteroid)
- Local infection:
- Incision and drainage
- Wound dressing
- Antibiotics
TREATMENT OF GENERALIZED EDEMA
Supportive:
1. Bed rest
- Decrease peripheral pooling
- Augment blood volume in central circulation
- Increases cardiac output, renal and hepatic perfusion
- Increases sodium diuresis
2. Sodium restriction
- 1-1.5 mEq/kg/day
- Avoid salty foods
3. Water balance
- Daily intake = Urinary loss + Insensible water loss
- When diuresis occurs, avoid water restriction
Diuretic therapy:
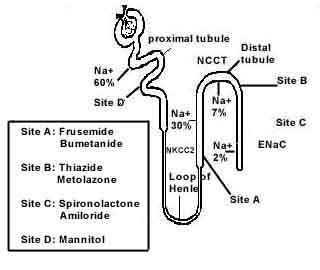
1. Loop diuretics (Furosemide/Lasix)
- 1-2 mg/kg/day (IV/IM/PO)
- Note: higher doses are required in acute glomerulonephritis or chronic renal impairment
- Side effects- hyponatremia, hypokalemia, metabolic alkalosis
2. Hydrochlorothiazide
- In steroid resistant Nephrotic syndrome
- 0.5-2 mg/kg/day P.O.
3. Spironolactone
- Initial therapy in edema of liver cirrhosis
- 1 to 3 mg/kg/day P.O.
Specific treatment:
1. Nephrotic syndrome:
- Prednisolone
- 1st 6 weeks: 2mg/kg/day on daily basis
- Next 6 weeks: 1.5 mg/kg/day; morning dose on alternate days
- Nephrotic diet
- IV albumin (sodium poor; slow infusion) with diuretics for severe oedema
- Steroid sparing agents in steroid dependent/resistant cases
2. Acute Glomerulonephritis:
- Diuretics (first line)
- I.V. Anti-hypertensives (Nifedipine, Diazoxide)
- Dialysis in severe cases
- Treat underlying cause
3. Chronic liver disease:
- IV albumin with diuretics for severe oedema
- Liver failure management
4. Cardiac failure:
- Diuretics
- Salt and fluid restriction
- Digoxin
- Treat arrhythmias
5. Cow’s milk allergy:
- Avoid cow’s milk
- Consider soy based formula
- Treat iron deficiency
6. Gluten hypersensitivity:
- Gluten free diet
- Treat iron deficiency
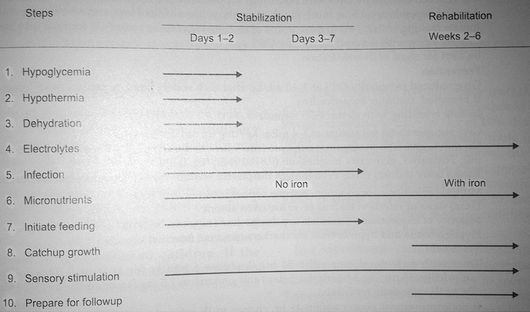
7. Malnutrition:
SUMMARY
- Localized edema is commoner than Generalized
- Commonest cause of edema in children:
- Generalized: Idiopathic nephrotic syndrome
- Localized: Allergic reaction
- Most children will have a benign diagnosis and self-limited course
- General measures for treatment include management of primary disease, bed rest, Na+ restriction and Diuretic administration.
- Most reliable index of progression of treatment of edema is daily alteration of body weight.
CONTRIBUTORS
2nd Batch, KIST Medical College
Shraddha Shrestha
Shuveccha Pandey
Srijana Shakya
Sulabh Shrestha
Surakshya Raymajhi
Nice one..it will help me out in tommrow lecture bcx i hv to present d history..thanks once again..
It was so on point and useful
Nice.
nice it will help me to do my presentation tomorrow well sumurised
Very good and theory as well as practically for both.
Well described.
Perfect summary