Synonyms: Faget sign, Sphygmo-thermic dissociation, Sphygmo-thermal dissociation
Definition of Relative Bradycardia
Physiologically, for each 1 °F rise in body temperature, there is a commensurate increase in the heart rate of 10 beats/min . When temperature elevations are not accompanied by a physiologic increase in the pulse, the patient is said to have a pulse-temperature deficit.
However, the term ‘relative bradycardia’ should only be applied to patients with temperatures in excess of 102 ° F since the difference between pulse and temperature readings of ≤ 102 ° F is insufficient to discern pulse temperature abnormalities.
Diagnosis of Relative Bradycardia
Criteria for using relative bradycardia in clinical diagnosis:
- Age of patient >= 13 years
- Temperature >= 102°F and <= 106°F
- The pulse is taken simultaneously with the temperature.
- The patient has normal sinus rhythm with no arrhythmias, second or third degree heart block, or pacemaker.
- The patient must not be taking beta-blockers.
Calculation of Expected pulse rate:
a. Method 1:
- Subtract 1 from the last digit of the farenheit temperature, multiply by 10, and then add the number to 100.
- Example: 103°F = (3-1) X 10 + 100 = 120/min
- Any pulse <120/min with a temperature ≥103°F is considered relative bradycardia.
b. Method 2:
- Multiply farenheit temperature by 10 and subtract 910 from it.
- Example: 103°F = (103 X 10) – 910 = 120/min
c. Method 3:
- Just use the unitary method.
- Add 10 for each 1°F above 102°F to 110
- Example: 103°F = 110 + 10 = 120
Appropriate temperature-pulse relationship:
| Temperature | Pulse in Beats per Minute |
| 102°F (38.9 °C) | 110 |
| 103°F (39.5 °C) | 120 |
| 104°F (40.0 °C) | 130 |
| 105°F (40.6 °C) | 140 |
| 106°F (41.1 °C) | 150 |
Causes of relative bradycardia
a. Infectious:
- Flavivirus:
- Dengue fever
- Yellow fever
- Bacteria:
- Salmonella typhi
- Salmonella paratyphi
- Leptospira
- Brucella
- Chlamydia psitacci
- Chlamydia pneumoniae
- Ricketssia prowazeki (epidemic typhus)
- Coxiella burnetti (Q fever)
- Ehlrichia chafeensis
- Legionella
- Parasites: Malaria
b. Non-infectious:
- Rise in ICP (Cushing’s reflex):
- Brain abscess
- Meningitis
- Brain tumors
- Pontine hemorrhage
- Other: Lymphoma, Drug fevers
Aids to Diagnosis
- Pneumonia + Relative bradycardia = Think of Atypical pneumonia (Legionella, Q fever, Chlamydia pneumoniae)
- Hospitalization + Multiple drugs for treatment + Other causes of fever excluded + Relative bradycardia = Think of Drug fever
- Rashes + Relative bradycardia = Think of Typhus or RMSF
- Hemorrhagic rash + Systemic toxemia + Relative bradycardia = Think of viral hemorrhagic fever
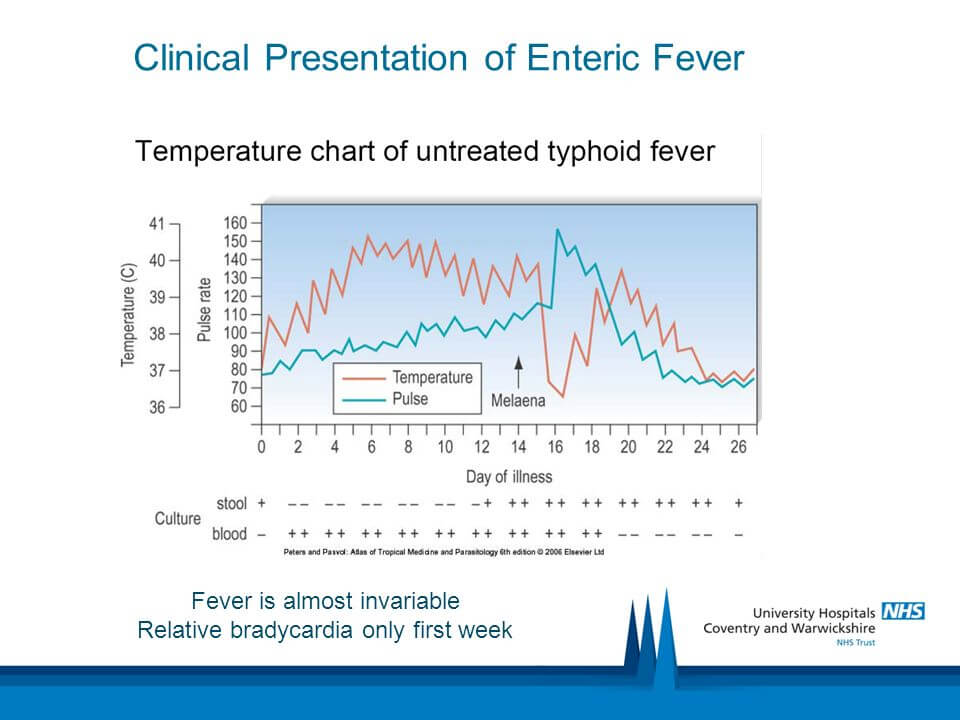
- Headache + Constipation/Diarrhea + Cough + Relative bradycardia = Think of 1st week of enteric fever
References:
- Hospital Medicine edited by Robert M. Wachter, Lee Goldman (MD.), Harry Hollander
- Infectious Disease Secrets By Robert H. Gates
- Infectious Diseases in Critical Care Medicine By Burke A. Cunha
- Cunha, B. A. (2000), The diagnostic significance of relative bradycardia in infectious disease. Clinical Microbiology and Infection, 6: 633–634. doi:10.1046/j.1469-0691.2000.0194f.x