Thomas test
Synonym: Hip flexion contracture test, Iliacus test, Iliopsoas test
Fixed flexion deformity of the hip and anterior pelvic tilt leads to a compensatory hyperlordosis of the lumbar spine to restore the body’s center of gravity. Compensatory hyperlordosis can mask the fixed flexion deformity of hip.
Thomas test:
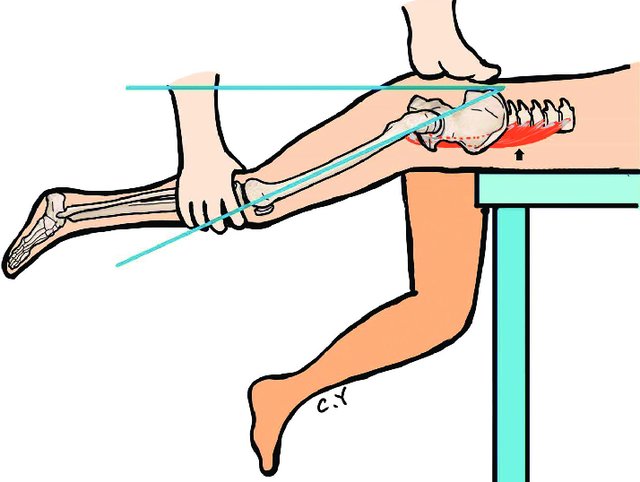
With the patient lying supine on the examination table, the knee and hip on the “good” side are flexed until the lumbar lordosis disappears and the knee is held against the chest. One hand is placed behind the lumbar spine (between it and the couch) to assess the degree of lumbar lordosis. If there is no lordosis when the affected limb lies flat on the couch there can be no fixed flexion deformity and there is no need to proceed with the test. The examiner then passively extends (presses down) on affected side thigh until ASIS begins to move forward. The angle of thigh to the bed is the angle of fixed flexion deformity (FFD).
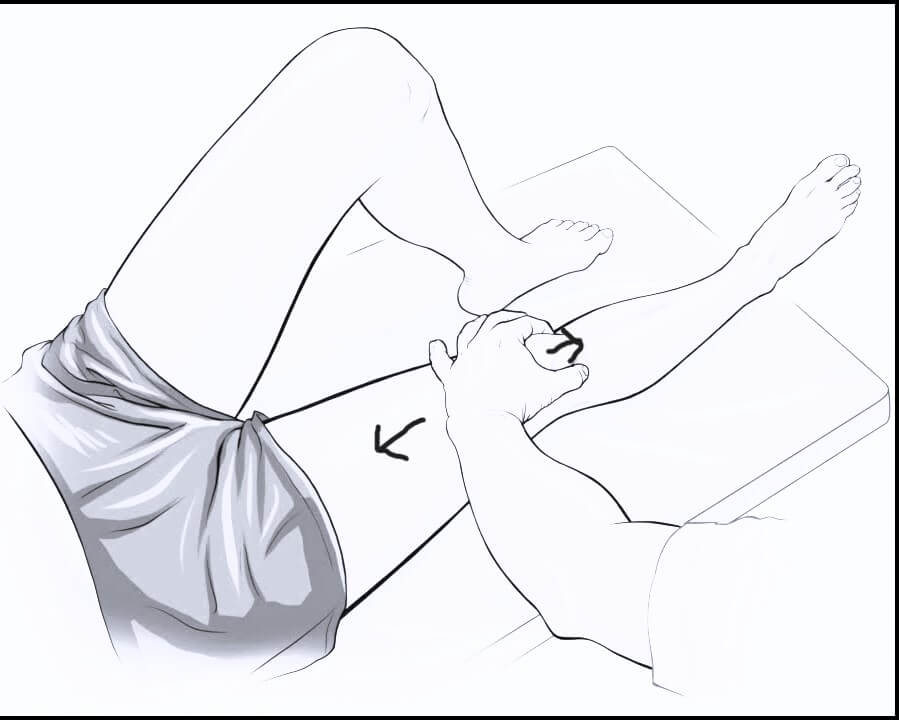
Alternatively, with the patient supine, both hips are flexed simultaneously to their limit – ask the patient to bring both knees up to their chest to achieve this. Ensure that the lumbar lordosis is obliterated by placing your hand under the lumbar area of the patient’s back. Place your other hand on one knee to keep it in position, lower the contralateral leg to a straight position.
An important aspect of this test is to obtain the zero set point for the lumbar spine. Patients with hyperlaxity or connective tissue disorders could have a false-negative result. In these patients, the zero set point can be established with an abdominal contraction.
Interpretation:
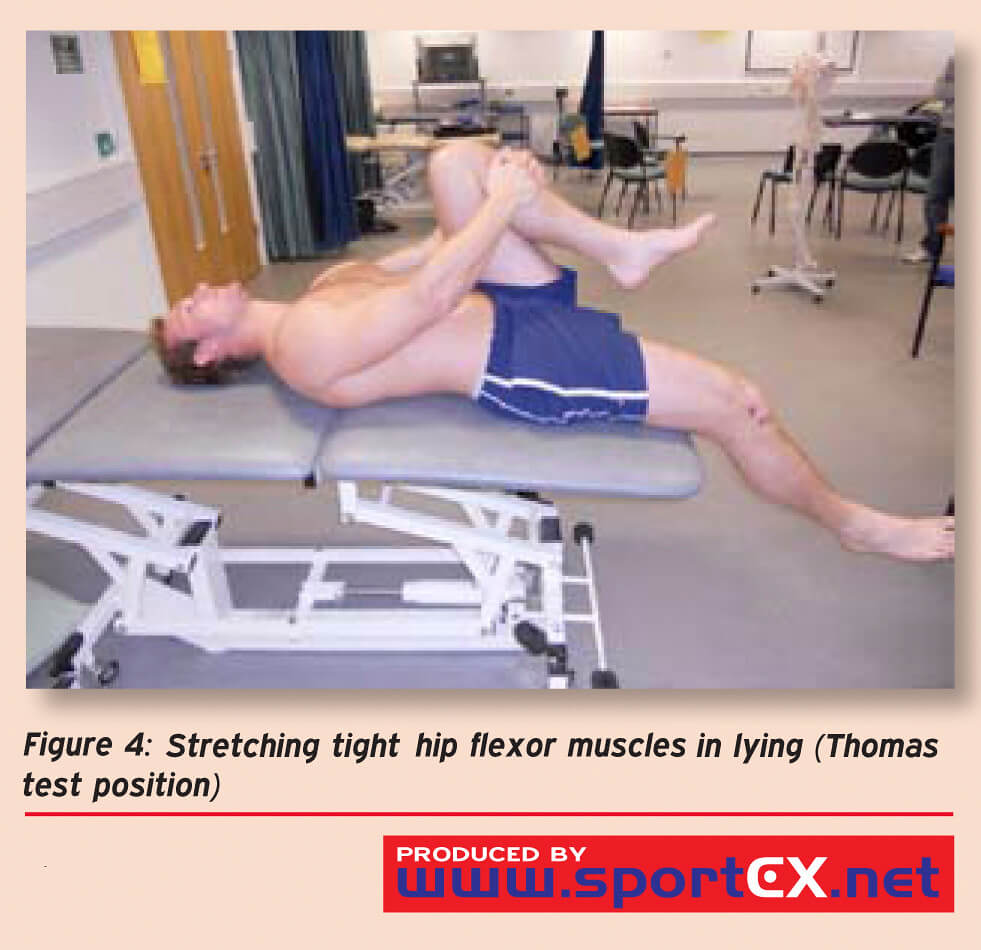
a. Positive test: Opposite thigh is raised off the surface of table (flexion contracture can be quantified by the angle of flexion of hip against the surface of table)
b. Negative test: Opposite thigh and leg remains in contact with the examination table
Mechanism of Thomas test:
Drawing up the knee and flexing one side of the hip rotates the pelvis upwards. In order to keep the alternate leg flat on the examination table, the hip flexors and rectus femoris must be supple and stretch enough to allow the leg to lie flat. If these are shortened, the hip cannot remain extended.
Modified Thomas test:
The modified Thomas test is similar, however it is performed on the edge of a table or surface.
a. Normal: Opposite thigh should be parallel with the bed, in neutral rotation and neither abducted nor adducted, with the lower leg being perpendicular to the thigh and in neutral rotation.
b. Iliopsoas contracture: Unable to have neutral angle of hip
c. Rectus femoris contracture: Unable to have 90 degrees of knee flexion
d. TFL/ITB contracture: Unable to have 15 degrees of hip abduction
Staheli test (Prone hip extension test)
The Staheli test is performed with the patient in the prone position on the edge of the examination table. The examiner places one hand on the pelvis and gradually extends the thigh with the other. The point at which the pelvis begins to rise indicates the end of hip motion and beginning of movement at the spine. At this point, the horizontal-thigh angle is measured.
It can be used for bilateral hip pathology.