Indications
- Transverse or dorsally angulated traumatic amputations of the fingertip involving exposed distal phalanx
- Tissue loss distal to the lunula (Zone I and Zone II finger-tip injuries)
Contraindications
- Volar-oblique (angulated) traumatic amputations
- Extension of the soft tissue loss proximal to the lunula (Zone III finger-tip injuries)
- Need for the proximal extent of the flap to originate proximal to the distal interphalangeal joint (digits 2-5) or the interphalangeal joint of the thumb
Advantages
- Preservation of nail length and potential for minimizing hook nail deformity
- Preservation of sensation and length, and good soft tissue coverage
Disadvantage
Tension (maximum tension occurs in mid portion of the defect) especially with large defects
Blood supply of flap
Oblique terminal branches of the digital arteries arising from the trifurcation of distal interphalangeal joint (a subcutaneous pedicle flap)
Technique
- Smooth or trim distal phalanx using a rounger if protruding
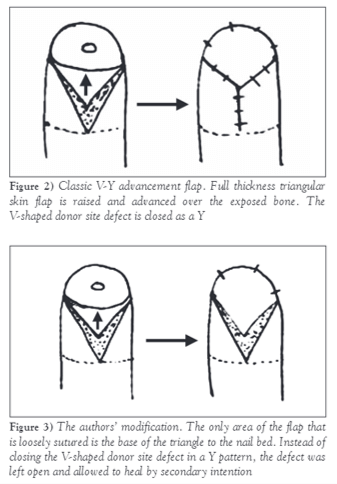
- Create a triangular-shaped flap:
- Depth: Full-thickness of skin (do not undermine flap – flap becomes avascular)
- Base: At the cut edge of skin distally (width should be same as the greatest width of the amputation)
- Tip: At level of distal interphalangeal flexion crease (crossing the crease can lead to flexion contracture)
- Advance the flap over the defected area and suture it to the nail bed with either 5-0 or 6-0 nylon sutures (Upto 1 cm advancement can be expected with adequate release)
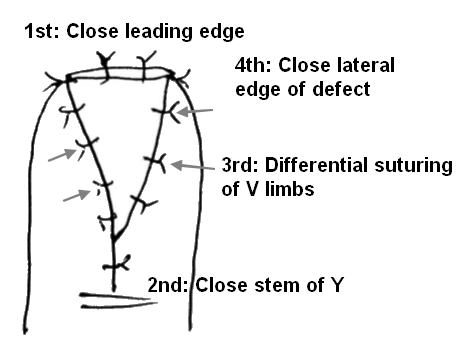
- Place corner stitches to avoid interference with the blood supply to the corners. Convert the V-shaped defect into a final Y-shaped wound.
- 1st: Suture the leading edge
- 2nd: Close the stem of Y
- 3rd: Differential suturing taking thin bites (epidermis) on V limbs
- Final: Suturing on lateral aspect of defect
- Proximal sutures may be placed, but if the flap appears ischemic after tourniquet release, then the proximal incision may be left open to heal secondarily.
References:
- The V-Y Plasty in the Treatment of Fingertip Amputations – American Family Physician (aafp.org)
- Netscher, D., Stephenson, J. (2015). Fingertip Amputations: Coverage, Local and Regional Flaps. In: Rozmaryn, L. (eds) Fingertip Injuries. Springer, Cham. https://doi.org/10.1007/978-3-319-13227-3_6
- https://youtu.be/ZwrbhW_1mnU