1. Provides optimal environment for fracture healing:
- Limits surgical dissections and avoids disruption of fracture hematoma (not exposing fracture site and indirect fracture reduction)
- Preserves periosteal blood supply (acts as internal external fixators)
- Avoids stress shielding below the plate (prevents local bone necrosis and improves ability for resistance to infection)
2. Relative stability of fracture:
- Most fractures repaired with MIPO techniques heal in condition of relative stability (fracture strain between 2-10%)
- Secondary bone healing with callus is favored in such condition.
3. Acts as internal fixator:
- Locking plates differ from nonlocking plates because stability is not dependent on the frictional forces generated at the bone–plate interface.
- Locking the head screw into the plate hole confers axial and angular stability of the screw relative to the plate. Because the stability of the construct does not depend on frictional forces generated between plate and bone, the bone–screw threads are unlikely to strip during insertion.
- With the screwhead locked in the plate, screw orientation is fixed to the plate resulting in a single beam construct functioning as an internal fixator.
- With the fixed‐angle and the screw locked in the plate, no movement at the plate screw interface is allowed, resulting in a decreased risk of screw pullout and screw loosening.
4. Plate length and Number of screws in Bridge plate function:
- Plate span ratio = Plate length/Segmental length of fractured or comminuted bone (the length increases the pullout force acting on the screw because of long lever arm for each screw)
- Plate screw density = Number of screws inserted/Number of screw holes on plate
- Comminuted fractures: <0.4-0.5
- Simple fractures: 0.3-0.4
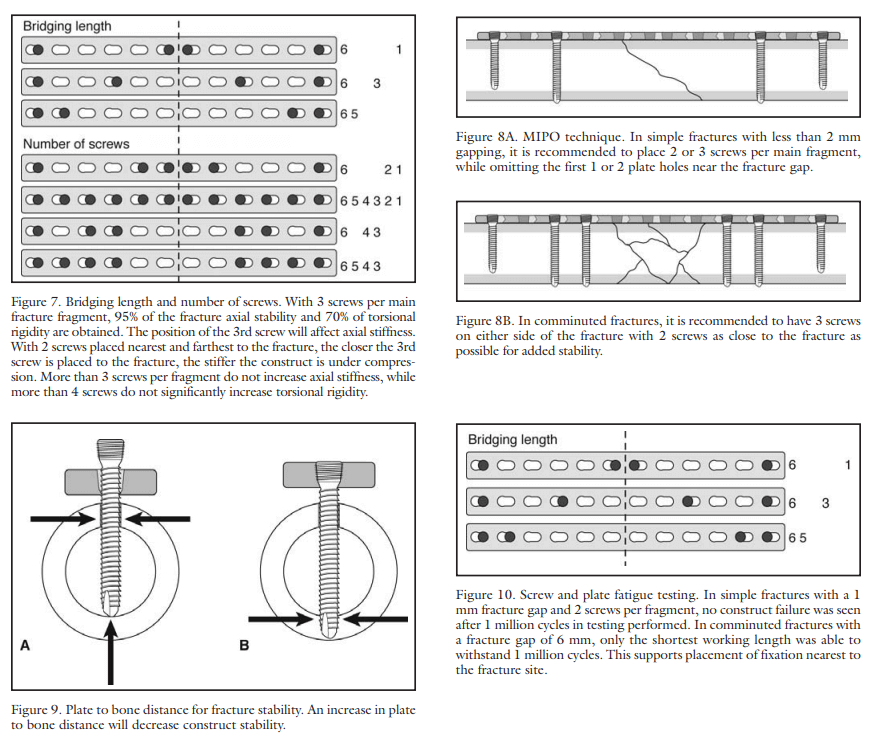
- Number of screws:
- Simple fractures: 2-3 screws per main fragment while omitting the 1st 1-2 holes near the fracture gap
- Comminuted fractures: 3 screws on either side of the fracture with 2 screws as close to the fracture as possible for added stability
- More than 3 screws per fragment do not increase axial stability
- More than 4 screws per fragment do not increase rotational stability
5. Plate working length:
- The plate working length is defined as the distance between the distal and the proximal screw nearest to the fracture.
- Recommendations aim toward increased plate working length in order to reduce axial stiffness of the construct and to allow interfragmentary movements.
- The plate working length in comminuted fractures might not be equal to the distance between the screws closest to the fracture, but rather to the unsupported area of the plate, which correspond to the length of the fracture gap.
References:
- 15475843.pdf (orthobullets.com)
- Layout 1 (podiatryinstitute.com)
- https://veteriankey.com/minimally-invasive-plate-osteosynthesis/

He is the section editor of Orthopedics in Epomedicine. He searches for and share simpler ways to make complicated medical topics simple. He also loves writing poetry, listening and playing music. He is currently pursuing Fellowship in Hip, Pelvi-acetabulum and Arthroplasty at B&B Hospital.