Wilm’s tumor is the most common primary renal tumor of childhood.
Origin: Embryonic nephrogenic (mesodermal) cells
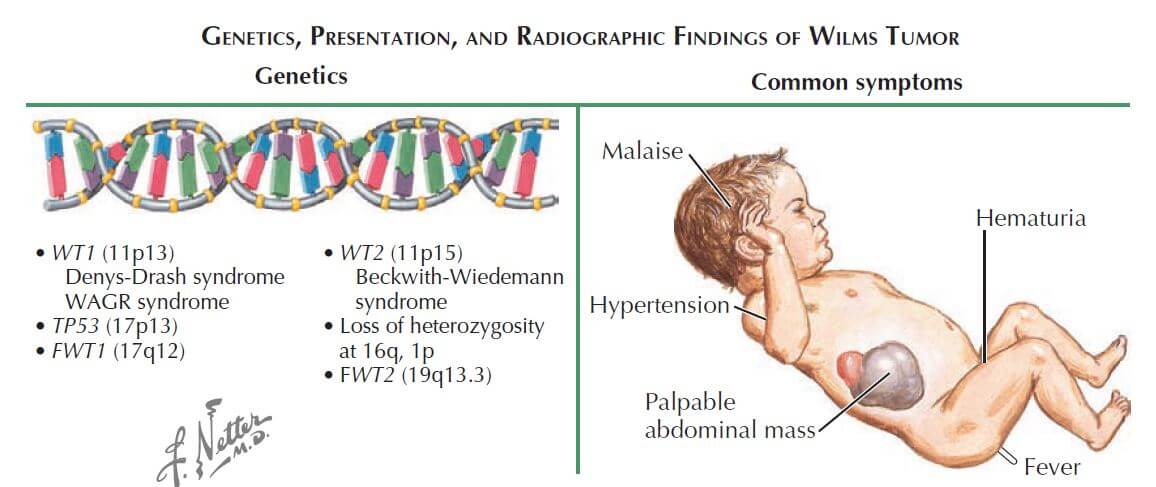
Mechanism: Deletion of WT-1 gene on chromosome 11
Pathology:
a. Macroscopic (Gross): large, solitary tan to grey color mass; pale on cut section with areas of hemorrhage; 10% are bilateral or multicentric; grossly difficult to distinguish from neuroblastoma
b. Microscopic: tumor containing 3 elements –
- Metanephric blastema
- Epithelial elements (Immature glomeruli and tubule)
- Stroma
Incidence: 1 per 10,000 children before the age of 15 years
Average age at diagnosis: 3-4 years
Symptoms:
- Usually asymptomatic abdominal mass (classic history – found during dressing or bathing)
- 20% patients present with minimal blunt trauma to mass
- Other: abdominal mass, gross hematuria, fever
Signs:
- Abdominal mass (mostly donot cross the midline)
- Hematuria (10-15%; indicates invasion of collecting system)
- Hypertension (20%; related to compression of juxtaglomerular apparatus)
- Signs of Beckwith-Wiedemann syndrome may be present
Associated syndromes:
Approx. 10% of Wilms tumors occur in children with syndromes.
1. WAGR syndrome (deletion of WT1 gene)
- Wilms tumor
- Aniridia
- Genitourinary (GU) anomalies
- Intellectual disability (mental Retardation)
2. Beckwith-Wiedemann syndrome (mutations of WT2 gene)
Others: Denys-Drash syndrome (WT1), Fraiser syndrome (WT1), Neurofibromatosis
Best initial test: Ultrasonography of abdomen
Diagnostic radiological tests: Abdominal and chest CT –
- Staging purpose
- Preoperative assessment
- Look at the contralateral kidney
Staging:
- Stage I: Limited to kidney and completely resected
- Stage II: Extends beyond kidney but completely resected; capsule invasion and perirenal tissue may be involved
- Stage III: Residual non-hematogenous tumor after resection
- Stage IV: Hematogenous metastases (lung, distal lymph nodes and brain)
- Stage V: Bilateral renal involvement
Best indicators of survival:
- Stage
- Histologic subtype: 85% have Favorable Histology (FH) with overall survival of 85% for all stages; 15% have Unfavorable Histology (UH)
Treatment:
Radical resection of affected kidney followed by:
- Lower grade tumors (I and II): Chemotherapy (Actinomycin D, i.e. DACT and Vincristine)
- Higher grade tumors (III and above): Radiotherapy
Routine pre-operative biopsy should be avoided as this upstages the tumor, requiring the intensification of chemotherapy and abdominal irradiation.
Neoadjuvant chemotherapy/radiotherapy may be required to regress the size of tumor before surgery.
This is a quick review of Wilm’s tumor on request of final year MBBS student Jaymala Shelke. For detailed information on Wilm’s tumor, refer to the textbooks.



Thank you for nice article.
I have 1 question, Is incidence of Wilms’ equal in both sexes or more in female child?
Here’s a quote from the book “Principles of Gender-Specific Medicine” by Marianne J. Legato – “Wilm’s tumor is slightly more frequent in girls than boys. Interestingly, the male:female ratio is 0.92:1 for unilateral tumors, and 0.60:1 for bilateral cases.”
Are you sure that is the most comum tumor in childhood? The most comum is a Central Nervous System, follow by leukemia and neuroblastoma, is not? Wilms is the most common renal tumor.
Thank you for the correction Vilani. Wilms is the most common childhood renal tumor.
having a doubt
” bilateral involvement without metastasis ”
Is this possible?
if possible means
what stage it is?
Approximately 5-7% of WT patients present with bilateral disease, either synchronously or metachronously. Bilateral WT usually occurs in younger children and more often in girls. Bilateral WT, Stage V is defined bilateral renal involvement at initial diagnosis. A much higher frequency of bilateral disease is observed in patients with predisposition syndromes.
Further reading:
1. Charlton J, Irtan S, Bergeron C, Pritchard-Jones K. Bilateral Wilms tumour: a review of clinical and molecular features. Expert Rev Mol Med. 2017 Jul 18;19:e8. doi: 10.1017/erm.2017.8. PMID: 28716159; PMCID: PMC5687181.
2. Özyörük D, Emir S. The management of bilateral Wilms tumor. Transl Pediatr. 2014 Jan;3(1):34-8. doi: 10.3978/j.issn.2224-4336.2014.01.04. PMID: 26835321; PMCID: PMC4728855.