Mechanism of Steroid Induced Leukocytosis
There are 3 major mechanisms responsible for corticosteroid induced granulocytosis:
1. Demargination of neutrophils from endothelial cells (60% of the rise):
- Recall the leukocyte adhesion cascade in the chapter of inflammation.
- L-selectins are present in leukocytes that mediates their rolling on the endothelial lining of the vessels.
- This relies on the balance between removal of L-selectins from cell surface by the enzyme cysteine-metalloproteinase (sheddase) and production of new L-selectins by the neutrophils.
- Steroids inhibit L-selectin synthesis at gene level, leading to demargination of leukocytes into the circulation.
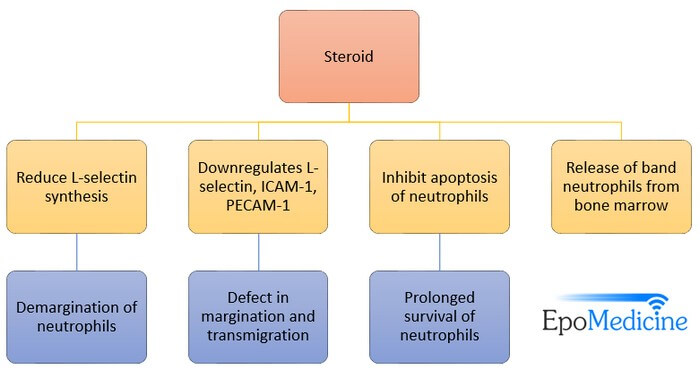
2. Delayed migration of PMNs into tissues and rate of apoptosis, i.e. improved survival (30% of the rise):
- During rolling, integrins are activated on the surface of leukocytes which bind to the ICAM-1 and PECAM-1 on the endothelial surface resulting in adhesion and trans-migration of leukocytes through the endothelial cells.
- Steroids down-regulate all these molecule, and the leukocytes are bound to stay in the circulation.
- Also, by unknown mechanism steroid inhibit apoptosis of leukocytes, prolonging their survival period.
3. Release of non-segmented (band) neutrophils from bone marrow (10% of the rise)
CBC findings in Corticosteroid Induced Neutrophilia
1. Mild to moderate leukocytosis with few cases reporting the counts as high as >20,000/cu.mm.
2. Not associated with a left-shift, i.e. predominance of band or unsegmented neutrophils (only 10% of rise is attributed to the release of band neutrophils from bone marrow).
3. Lymphopenia
4. Eosinopenia
5. Monocytosis
Leukocytic response with Corticosteroid
1. Average increases in WBC count have been reported to be approximately 4,000/mm3 in patients taking 40-80 mg of oral prednisone.
2. Leukocytosis is first noted a few hours of administration and reaches maximal intensity within 2 weeks of continued treatment after which the white cells decrease but not to the pre-treatment level.
3. The pattern of steroid induced changes in the total WBC, neutrophil, lymphocyte and eosinophil count is predictable during the first 3 days of initiation of treatment in absence of active infection at the time of admission.
4. Although the degree of leukocytosis may be related to the dosage administered, it may appear sooner with higher doses.
Differentiating Steroid induced Leukocytosis with Infection
During infection, unsegmented or band neutrophils are released from the bone marrow resulting in:
- Shift to the left in the peripheral white blood cells, i.e., more than 6 percent band forms
- Appearance of toxic granulation
These findings are rare in corticosteroid induced leukocytosis.
Other Common drugs responsible for Leukocytosis
- Beta agonists
- Lithium
- Anti-epileptics
References
1. A General Review of the Mechanisms for Steroid or Glucocorticoid Induced Increases in the White Blood Cell (WBC) Count – EBMconsult
2. Shoenfeld Y, Gurewich Y, Gallant LA, Pinkhas J. Prednisone-induced leukocytosis. Influence of dosage, method and duration of administration on the degree of leukocytosis. Am J Med. 1981 Nov;71(5):773-8. PubMed PMID: 7304648.
3. White Blood Cell Dynamics In Copd And Asthma Patients Treated With Corticosteroids – Pandya CM, Brateanu A. Chest. 2007;132(4_MeetingAbstracts):505c-506