Views
- AP pelvis: patient supine and the x-ray beam oriented 90 degrees to the patient’s long axis, passing through the patient from anterior to posterior
- Pubic symphysis and coccyx in straight line in middle of screen with 1-3cm between superior pubic symphysis and tip of coccyx
- Greater and lesser trochanters should be clearly distinguishable
- Obturator rings symmetric
- Additional views:
- Inlet and Outlet views: For pelvic ring fractures
- Inlet views: patient supine and the x-ray tube positioned at the patient’s head, angled 45 degrees (25 to 60 degrees) toward the patient’s feet. This allows assessment of pelvic brim integrity, AP displacement of the hemipelvis, internal or external rotation of the hemipelvis, and anterior displacement of the sacrum.
- Outlet views: patient supine, with the x-ray tube at the patient’s feet and angled 45 degrees (25 to 60 degrees) toward the head. This provides an excellent view of the sacrum, which is perpendicular to the x-ray beam in this position. The sacral neural foramina are seen well in this view, and vertical displacement of the hemipelvis may be evident.
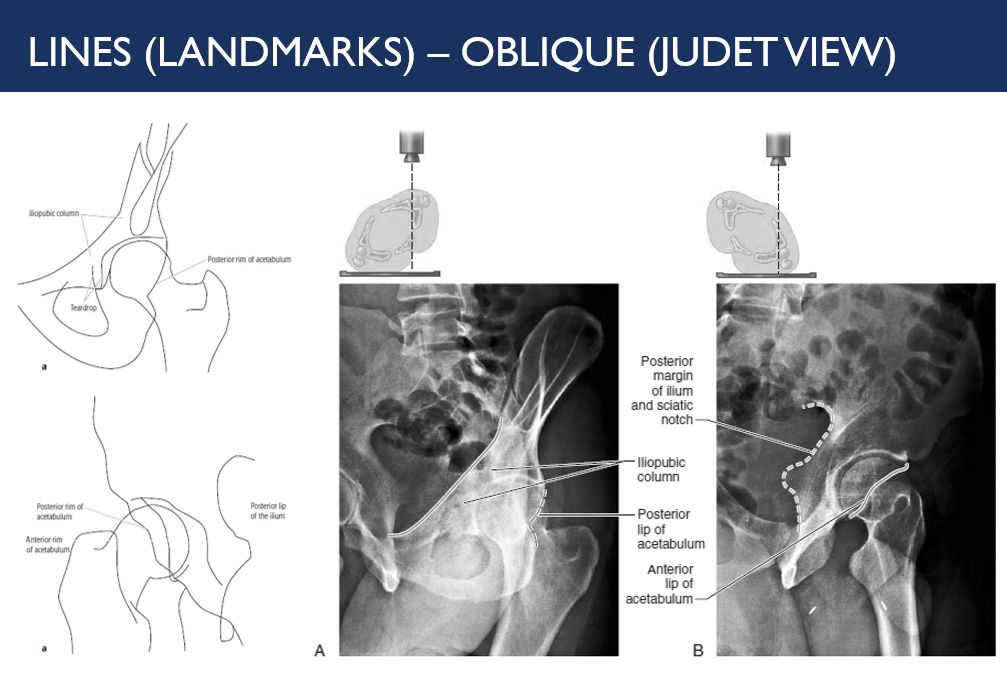
- Judet views (Oblique views): For acetabular fractures
- In the true frontal plane of a AP pelvis, the obturator segment and the iliac wing have an angulation of approximately 45 degrees. Thus, oblique views are taken for two-plane analysis with the pelvis rotated either right or left by 45 degrees.
- Iliac oblique: Rotated 45 degrees away from side of interest
- Obturator oblique: Rotated 45 degrees towards the side of interest
- In the true frontal plane of a AP pelvis, the obturator segment and the iliac wing have an angulation of approximately 45 degrees. Thus, oblique views are taken for two-plane analysis with the pelvis rotated either right or left by 45 degrees.
- Inlet and Outlet views: For pelvic ring fractures
Bones
Cortical outline and bony texture
a. Pelvis
- Ilium: iliac crest, anterior superior iliac spine, anterior inferior iliac spine
- Ischium: ischial tuberosity, ischial spine
- Pubis: superior pubic ramus, inferior pubic ramus
b. Hip
- Acetabulum: Trace 6 Letournel lines –
- Iliopectineal line: disruption suggests anterior column fracture
- Ilioischial line: disruption suggests posterior column fracture
- Acetabular roof (sourcil)
- Anterior rim
- Posterior rim
- Tear drop: displacement suggests occult acetabular fracture
- Femur: femoral head, femoral neck, greater trochanter, lesser trochanter
Rings
Pelvis is often conceptualized as a rigid polo mint ring and a ring is disrupted at one place, one should look for disruption at another place as well.
- Trace the main pelvic ring
- Trace 2 obturator rings
- Trace sacral foramina
Lines
- Pelvis and Acetabulum: Look for 6 Letournel lines as described earlier
- Hip:
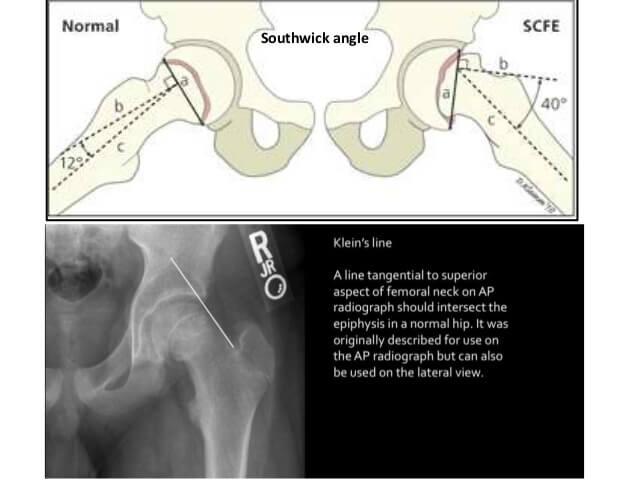
- Klein line: If the line along superior femoral doesn’t intersect femoral head, think of SCFE
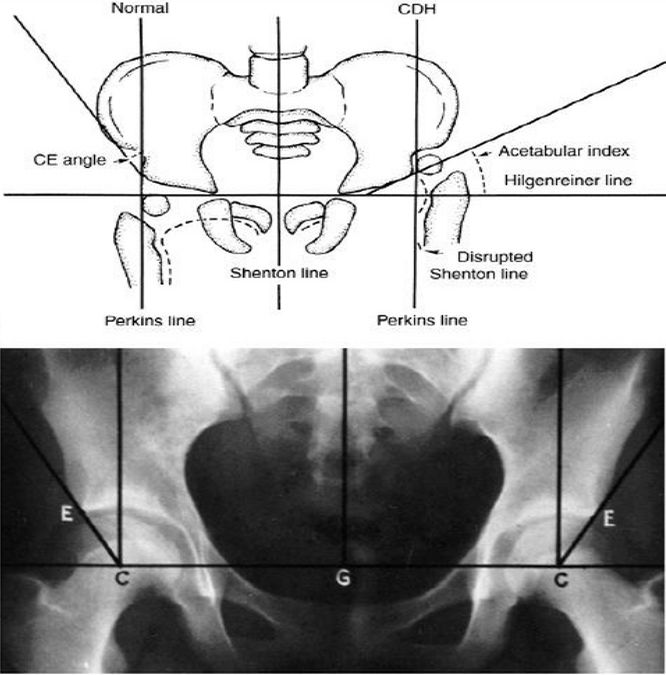
- Shenton’s line: Disruption of arc formed by undersurface of superior pubic ramus and medial femoral cortex indicates femoral neck fracture or DDH
- Hilgenreiner line: Horizontal line through triradiate cartilage of acetabulum – femoral head ossification must be below this line
- Perkin’s line: Vertical line (perpendicular to Hilgenreiner’s line) from the lateral margin of ossified acetabular roof – femoral head ossification must be medial to this line
- Trabeculae: 5 groups of trabeculae in proximal femur
- Principal groups:
- Tensile: Head to Tension side (lateral surface)
- Compressive: Head to Compression side (medial surface)
- Secondary groups:
- Tensile: Below greater trochanter (tension side)
- Compressive: Greater trochanter to lesser trochanter (compression side)
- Greater trochanteric
- Ward’s triangle: Formed by Primary tensile and compressive and secondary compressive trabeculae (weak zone)
- Babcock’s triangle: Area between primary compressive and tensile group in subcapital region – watershed between femoral and obturator circulation (common locus for origin of TB hip)
- Principal groups:
- Intertrochanteric crest: Delineates between intracapsular region proximally and extracapsular region distally
Angles
- Acetabular angle: Angle formed by line intersecting most superolateral aspect of acetabular roof and –
- Adults: Inferior margin of tear drop (>47º = acetabular dysplasia)
- Children: Higenreiner line (>22º beyond 1 year = DDH)
- Center edge angle of Wiberg: Angle between vertical line from center of femoral head to and line between edge of acetabulum to center of femoral head – <20 degrees is considered abnormal (reliable only in >5 year old)
- Roof arc angle: Roof arc angle is a method to evaluate adequate acetabular coverage and stability of the femoral head, Matta and Merritt study based on clinical findings and suggested that the fracture crosses acetabular weight bearing dome when <45° medial, anterior and posterior roof arc angles.
- vertical line is drawn to the geometric center of the acetabulum
- another line is drawn through point where fracture line intersects acetabulum & again to geometric center of the acetabulum;
- angle drawn in this way represents medial, anterior, or posterior roof arc as seen on AP, obturator oblique, or iliac views, respectively
Joints
- Sacroiliac: 2-4 mm, equal bilaterally
- Pubic symphysis: <5 mm
- Hip (femoral/acetabular): 3-5 mm
- Femoral head superolateral to joint space and appear smaller: Posterior dislocation
- Femoral head inferomedial to joint space and appear larger: Anterior dislocation
Soft tissues
- Fat pads: These fat pads do not lie against the joint capsule directly and thus are not displaced outwardly if fluid accumulates within the joint but can be moved outwardly and obliterated secondary to edema around the hip joint.
- Iliopsoas fat pad: Inferior to femoral neck
- Gluteus fat pad: Superior to femoral neck
- Obturator internus fat pad: Medial to iliopectineal line
- Periosteal swelling