Immobilization Protocol
| Dorsal blocking orthosis | Early stage (0-3/4 weeks) | Intermediate stage (4-6 weeks) | Late stage (6-8 weeks) |
| Wrist: 20-30 degrees flexion MCP: 40-60 degrees flexion IP: Neutral | ROM of elbow and shoulder | Increase wrist extension (towards neutral) within splint Tendon gliding exercises (hold each position 3 seconds, repeat 10 times, do 3 sessions per day) – Straight – Hook fist – Full fist – Straight fist – Platform position | Discard splint Isolated joint blocking exercises of FDP and FDS |
Cast immobilization is necessary in children younger than 10 years of age due to lack of compliance with motion protocols.
Early Passive Motion Protocols
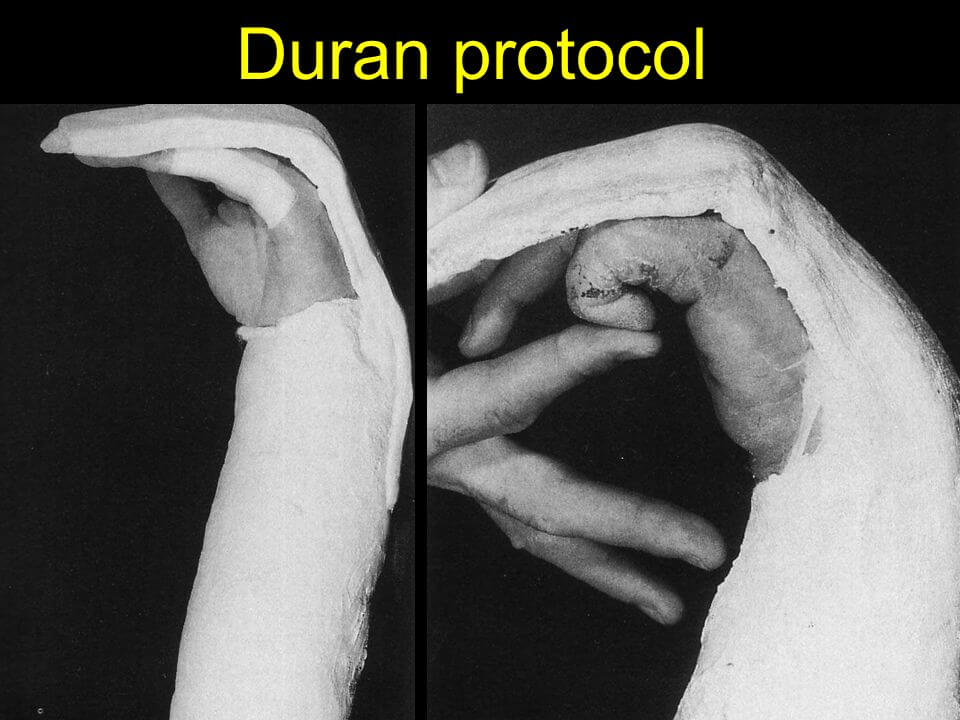
| Protocol | Kleinert | Duran | Modified Duran |
| Dorsal blocking orthosis | Involved finger secured with elastic thread or rubber band into full composite flexion | Fingers strapped into extension at night | |
| 1. Wrist flexion | 30 degrees | 20 degrees | -20 to +20 degrees |
| 2. MCP flexion | 40-60 degrees | Loose flexion | 40-50 degrees |
| 3. IP flexion | Neutral | Neutral | Neutral |
| Early stage (0-3/4 weeks) | Passive flexion (by rubber band traction) and active extension of fingers (repetitions: 10x per waking hour) | Passive DIP joint extension with MCP and PIP held passively in flexion; Passive PIP joint extension with MCP and DIP held passively in flexion (repetitions: 6-8x twice daily) | As in Duran + Composite passive finger flexion with active finger extension; Synergistic wrist and finger out of splint (only in therapy) |
| Intermediate stage (4-6 weeks) | Gentle active finger flexion is initiated | Splint is replaced with a wrist band and traction to prevent simultaneous finger and wrist extension; Gentle active finger flexion is initiated | Gentle active finger flexion is initiated |
| Late stage (6-8 weeks) | Resisted exercises are initiated | Resisted active finger flexion | Resisted active finger flexion |
Early Active Motion Protocols
There are many protocols for EAM including Gratton, Strickland, Tang, etc. Here, we will be discussing MGH protocol.
Day 1:
- Dorsal blocking splint: Wrist neutral, MCP 70 degrees, IP neutral
- Modified Duran
- Place and hold exercises (passively flex digits and allow patients to actively contract muscles to hold digits in fist – composite and differential)
3 week:
- Gentle tenodesis exercises out of splint
- Continue place and hold exercises
4 week:
- Active composite flexion exercises out of splint
- Differential tendon gliding exercises
- No passive extension, no blocking
- Continue dorsal blocking splint between exercises
5 week:
- Initiate blocking exercises
- Splint at night and for protection only during the day
6 week:
- Discontinue splint
- Initiate passive extension
7 week:
- Start composite passive extension
8 week:
- May start light strengthening
12 week:
- Normal activities
References:
Grabb and Smith’s Plastic Surgery – 7th Edition
https://repository.up.ac.za/bitstream/handle/2263/61677/Wentzel_Comparison_2017.pdf