Synonyms: Nosebleed, Nasal bleeding
Definition: Epistaxis is defined as bleeding from the nasal cavity. It ranges from minor blood-tinged mucus when blowing the nose to life-threatening hemorrhage.
Epidemiology:
- Age: Bimodal distribution – common in <10 years and >60 years
- Season: Winter
Anatomy and Physiology:
Why is the nose prone to bleeding?
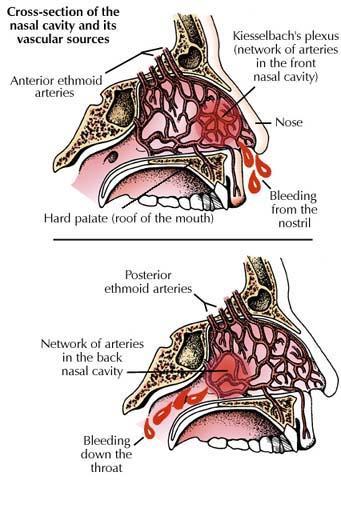
Nose is a highly vascular organ with a large surface area secondary to intense heating and humidification requirements which also predispose it to bleeding. The peculiar features of the vascular supply of nasal cavity are:
- Vasculature runs just under mucosa, which is not a squamous epithelial tissue
- Several arterial and venous anastomoses
- Receives blood from the territories of the external and internal carotid arteries
Arterial supply of the nasal septum:
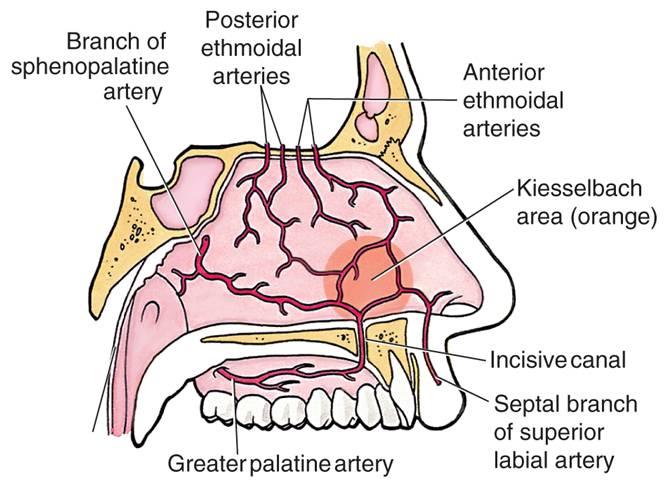
The region above the root of the middle turbinate is supplied by the anterior and posterior ethmoidal arteries, these are branches of the ophthalmic artery (internal carotid), with the remaining areas being supplied by the sphenopalatine, greater palatine and superior labial branch of facial artery (external carotid). The sphenopalatine artery is considered to be the main arterial supply of the nasal cavity and originates from the maxillary artery. The posterior ethmoidal artery may be absent in 30% of noses.
Summary:
Internal carotid system (Above the root of middle turbinate):
- Anterior ethmoidal artery (from ophthalmic artery)
- Posterior ethmoidal artery (from ophthalmic artery)
External carotid system (Below the root of middle turbinate):
- Septal branch of sphenopalatine artery (terminal branch of maxillary artery)
- Greater palatine artery (from maxillary artery)
- Septal branch of superior labial artery (from facial artery)
Venous supply of the nasal septum:
The veins generally follow the arteries, but additional emissary veins connect the venous drainage to the cavernous plexus. A relatively common finding is a prominent retrocolumellar vein that runs parallel to the columella adjacent to the mucocutaneous junction.
Sites of Bleeding:
| Site of Bleeding | Little’s area or Kiesselbach’s plexus | Woodruff’s plexus | Retrocollumelar vein |
| Incidence | 90%; Children and young adults | 10%; Elderly and hypretensives | Young people (<35 years) |
| Results in | Anterior epistaxis | Posterior epistaxis | Venous epistaxis |
| Location | Antero-inferior region of nasal septum, just above the vestibule | In the lateral nasal wall, inferior to the posterior end of inferior turbinate | 2mm behind the columella at the anterior edge of the little’s area |
| Anastomosis | Anterior ethmoidal artery + Superior labial artery + Sphenopalatine artery + Greater palatine artery (All that supplies nasal septum except posterior ethmoidal artery) | Posterior nasal artery + Sphenopalatine artery + Ascending pharyngeal arteries (All are branches of internal maxillary artery belonging to ECA system) | |
| Features | Nasal mucosa is very fragile and is tightly adherent to the underlying cartilage and thus offers little resistance to mechanical or functional stress – so easily irritated by nasal picking, cold dry air, cigarette smoking | The plexus is venous in origin and have no muscle walls leading to poor hemostasis. | Crosses the nasal floor and anastomose with the plexus of lateral nasal wall.
Also, the commonest site of nose picking. |
Note: Another common site of bleeding is Browne’s area which is situated on the posterior part of the nasal septum.
Classification and Causes of Epistaxis:
A. Primary or Secondary Epistaxis:
1. Primary (Idiopathic): 70-80%
2. Secondary (Proven casual factor):
| Local (Nose) | General |
Trauma:
|
Cardiovascular:
|
Nasal or sinus infections:
|
Blood and blood vessels:
|
Nasal or sinus neoplasms:
|
Liver disease: Liver cirrhosis |
| Deviated nasal septum | Renal disease: Chronic Kidney Disease |
Iatrogenic:
|
Drugs:
|
Environmental:
|
Mediastinal tumors: Increases venous pressure in nose |
Medicinal:
|
Acute general infection:
|
| Vicarious menstruation |
B. Adult or Childhood Epistaxis:
- Childhood epistaxis: <16 years
- Adult epistaxis: >16 years
C. Anterior or Posterior Epistaxis:
| Anterior Epistaxis | Posterior Epistaxis | |
| Incidence | More common (90%) | Less common (10%) |
| Source | Anterior to the plane of piriform aperture | Posterior to the plane of piriform aperture |
| Blood flows | Out from the front of nose | Back into the throat |
| Age | Children or young adults | >40 years |
| Localization | Easy | Difficult |
| Common site | Little’s area | Woodruff’s plexus |
| Common cause | Trauma | Spontaneous – Hypertension or arteriosclerosis |
| Severity | Less severe | Severe |
| Treatment | Usually controlled by local pressure or anterior pack | Requires hospitalization and posterior nasal pack is often required |
Common causes by age:
- Children: Nose picking, Foreign body, Exanthematous fever, Nasal diphtheria
- Adolescent: Nasopharyngeal angiofibroma, Traima, Sinusitis
- Adults: Sinusitis, Trauma, Idiopathic
- Middle age: Tumors
- Elderly: Hypertension, Malignancy