Hilum in human anatomy refers to the depression where structures such as blood vessels and nerves enter an organ. The structures contributing to hilar shadows in a Chest X-ray are:
- Major: Pulmonary artery and veins
- Minor: Fat, Lymph nodes and Bronchial walls
Normal Hilum:
- Position: Left hilum is slightly higher than the right hilum
- Shape: Concave
- Size: Similar on both sides
- Density: Almost same on both sides
Approach to Analyzing the Hilum in Chest X-ray:
If the hilum appears abnormal, firstly re-evaluate for the rotation.
a. Analyze the position of hilum:
1. Identify main lower lobe pulmonary arteries: They can be compared to a little finger pointing downwards and medially. Sometimes, usually on the left side – it can appear only as the proximal phalanx of the finger.
Interpretation: If the little finger shadow of the right lower lobe artery is not seen then you must check for evidence suggesting collapse of the right lower lobe.
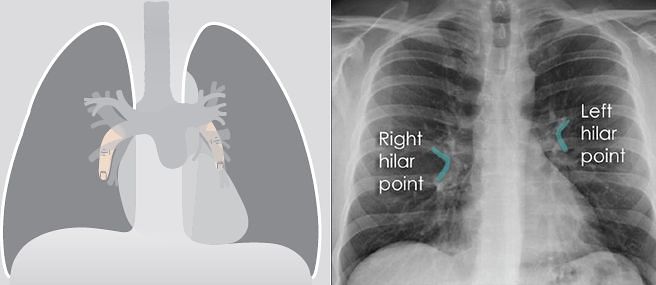
2. Identify the hilar point: Look for the site where the most superior upper lobe vessel – either vein or artery – crosses the lateral margin of the little finger. The point of crossing is known as hilar point and forms a horizontal “vee” (> or <).
Interpretation: The left hilum must never be lower than the right hilum. Whenever a left hilum appears lower than the right hilum – look for other evidence suggestive of:
- Collapse of either the left lower lobe or of the right upper lobe
- Enlargement of the right hilum
b. Analyze the density of hilum:
The presence of more than a slight difference in density raises the suspicion that there is abnormal tissue at the hilum — e.g. a hilar mass.
c. Analyze the enlargement of hilum (if present):
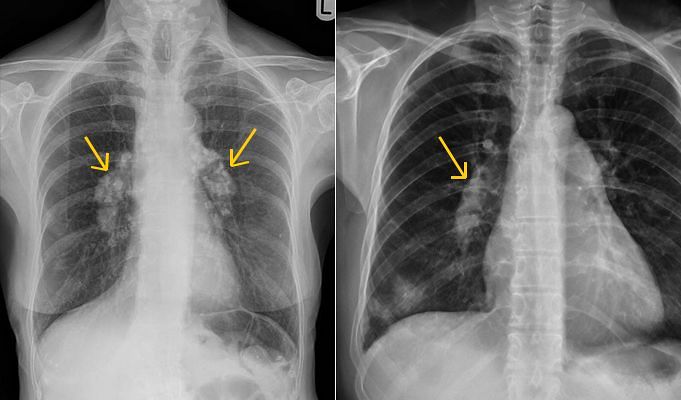
1. Lymph Node enlargement:
- Lobulated appearance
- Presence of calcification within the mass indicates lymph node enlargement usually tuberculosis. Egg shape calcification indicates lymphadenopathy due to silicosis.
2. Arterial enlargement:
- Can be traced into and are seen to be part of the “mass” – hilar mass
- Smooth margins
- In pulmonary arterial hypertension the arteries in the outer two-thirds of each lung are disproportionately smaller (diameter) than those at the hila (peripheral pruning)
Right: Pulmonary artery hypertension
3. Malignancy:
- Spiculated irregular or indistinct margins
- Hilar enlargement due to malignant lung lesion is also associated with superior mediastinal lymphadenopathy. Look at the lung fields (for presence of tumor) and bone/ribs for metastasis.
Causes of Hilar Enlargement:
Unilateral:
- Infection: tuberculosis, viral infection in children
- Vascular: pulmonary artery stenosis, pulmonary artery aneurysm
- Tumour: lymph nodes (metastases; lymphoma; bronchial carcinoma)
Bilateral:
- Sarcoidosis
- Tumour: metastases, lymphoma
- Vascular: pulmonary arterial hypertension (COPD; mitral valve disease; left to right shunt; recurrent pulmonary embolism)
- Infection: tuberculosis (occasionally)
Hilum convergence/bifurcation sign: Helps to analyze if the hilar enlargement is due to –
- Mass: If the vessels converge medial to the hilar shadow
- Vessels: If the vessels converge and merge directly on to the hilar shadow
Other signs of hilum:
Silhouette sign: This role of this sign is not just limited for the diagnosis of consolidation but to any mass lesion projected over a hilum.
- Hilar mass: Obscure the adjacent margin of the arteries at the hilum
- Mass – anterior or posterior to hilum: Margins stay unobscured
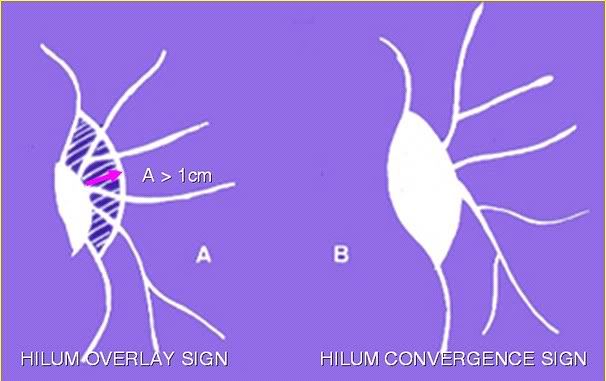
Hilum overlay sign: Cardiac enlargement vs Mediastinal enlargement
- Hilum pushed lateral to the lateral border of the “mass” — cardiac enlargement.
- Hilum smedial to the lateral border of the “mass” — mediastinal mass present.
I have had a chest X-ray and been told that there is a small consolidation projecting over the left hilum and no other significant abnormality.
My only symptoms are a persistent dry cough that has lasted for 3 months and a clear chest.
Can anyone elaborate on what this potentially means?
I Think you should search about TB
What is a circular structure over the left halium
After read Chest Xray their mentioned followings.Can i know what are the reasons for that? (ex: cancer)
There is prominent left hilum and it is more than expected denisity of the main pulmonary trunk.it is worth of doing CECT chest to out any hilar pathology.
Bilateral lung fields are clear.
No pleural effusion is seen.
I have a CXR after coughing 2 weeks. The report stated a slightly prominent L hilar shadow without significantly increase density. Also there was prominent bronchovascular shadow than other natures. Otherwise the lungs are clear.
I had on and off coughing for only ONE time a day (usually at noon time) with / without any sputum. This daily cough lasted for 4 months and seems to be subsided now. I have no fever or any other symptoms. What might be other differential diagnosis other than TB?
What is the Treatment for hilar prominence on my right side of Chest.I cheak of TB and Blood test all Reports are normal.I go oman Becouse of that he was give me unfit.
Pls,Reply as soon as Possible.
Thanking you.
Manish shukla
The most common causes of hilar prominence on chest radiographs are vascular engorgement and adenopathy. Unilateral hilar adenopathy may be related to pneumonitis or neoplasia. TB may be one of the most importants cause of asymmetric hilum particularly in developing coutries. Interpretation of unequal hilum depends on findings of detail history, meticulous clinical examination, and appropriate investigation.
What is a circular structure over the left hilum
In a normal condition, in the lateral view chest x-ray, the right and left upper lobe bronchi can be seen as two circular radiolucent areas with the right above the left.
Thank you for very interesting information! One additional question, my teen child has just had an episode of percieved obstruction/ chest pain. We had a chest x ray and the Dr said it showed bilateral increased density/ thickening of hilus, basically equal both sides but maybe a little more on the right side. The dr did not provide any explanations to this findings and Just recommended specialist care. In a child, what can this represent? Thanks so much!
In pediatric population, bilateral hilar enlargement can be due to misinterpretation of normal finding, lymphadenopathy or pulmonary artery dilation.
Lymphadenopathy – Bronchiolitis, Reactive airway disease, Measles, Pertussis, Cystic fibrosis, Lymphoma, Leukemia, Mycoplasma infection, Tuberculosis, Fungal infection, Bacterial pneumonia, Sarcoidosis
Pulmonary artery dilation – Congenital heart disease with left-to-right shunt, primary pulmonary hypertension, chronic pulmonary disease, pulmonary regurgitation, pulmonary venous abnormality
As the differentials are wide, it is necessary to correlate the findings clinically which can best be done by a Pediatrician.