Synonyms: Tonsils (Unless otherwise specified, tonsils usually refers to palatine tonsils), Faucial tonsils
Definition: Almond shaped, ovoid mass of lymphoid tissue situated bilaterally in the lateral wall of oropharynx within the tonsilar recess or sinus bounded by palatoglossal fold anteriorly i.e. anterior pillar and palatopharyngeal fold posteriorly i.e. posterior pillar. They belong to MALT (Mucosa Associated Lymphoid Tissue).
Size: Variable, 10-15 mm intransverse diameter and 20-25 mm in vertical dimension (larger in children)
Surface marking: An almond shaped area over the lower part of masseter muscle, a little above and in front of the angle of mandible marks the tonsil on the surface.
Parts:
A) 2 Surfaces:
1. Medial surface:
- Lined by non-keratinizing stratified squamous epithelium which is continuous with that of palatoglossal fold and tongue
- Mucosa invaginates into the substance of tonsil to form 12-15 tonsillar crypts
- Largest crypt known as crypta magna or intratonsillar cleft opens near the upper part (represents ventral part of 2nd pharyngeal pouch)
- Crypts increase the surface area of tonsil
2. Lateral surface:
- Covered by tonsillar hemicapsule formed by the condensation of pharyngobasillar fascia which extend into the tonsil to form septa that conduct nerves and vessels
- Tonsillar bed is separated from the capsule by loose areolar tissue which forms peritonsillar space
- Palatine/External palatine/Paratonsillar vein descends from palate in the loose areolar tissue
- Capsule is firmly attached anteroinferiorly to the side of the tongue, just in front of the insertion of palatoglossus and palatopharyngeus muscle
- Tonsillar artery enters near this firm attachment
B) 2 Poles:
1. Upper pole:
- Extends into soft palate
- Plica semilunaris: Semilunar fold of mucous membrane which extends from the anterior pillar to posterior pillar and covers the medial part of upper pole
- Supratonsillar fossa: Potential space enclosed by the semilunar fold
2. Lower pole:
- Attached to the tongue
- Triangular fold: of mucous membrane extends from anterior tonsillar pillar to the lower pole
- Anterior tonsillar space: Potential space enclosed by the triangular fold
- Tonsillolingual sulcus: separates tongue from the lower pole and is a seat of carcinoma
C) 2 Borders:
1. Anterior border: related to palatoglossal arch (anterior tonsillar pillar)
2. Posterior border: related to palatopharyngeus arch (posterior tonsillar pillar)
Bed of Tonsil:
From within outwards, tonsillar bed consists of:
- Pharyngobasillar fascia
- In upper and posterior part: Palatopharyngeus muscle
- In postero-superior 2/3 rd: Superior constrictor muscle
- In antero-inferior 1/3 rd: Styloglossus muscle accompanied by glossopharyngeal nerve (CN IX)
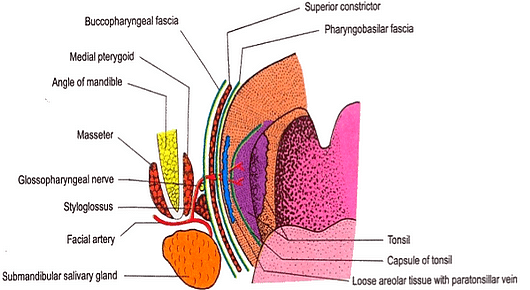
Relations of tonsillar bed:
- Arteries:
- Facial artery and it’s ascending palatine branch
- Ascending pharyngeal artery
- Internal carotid artery (lies about 25 mm behind and lateral to the tonsil)
- Styloid process (if enlarged)
- Submandibular salivary gland
- Medial pterygoid muscle
- Angle of mandible
Tonsils maintain its position:
- By the suspensory ligament of the tonsils it is connected with the tongue
- The palatoglossus and palatopharyngeus muscles attached to the fibrous capsules of the tonsils
- By the perivascular stalks
Arterial supply: 5 arteries
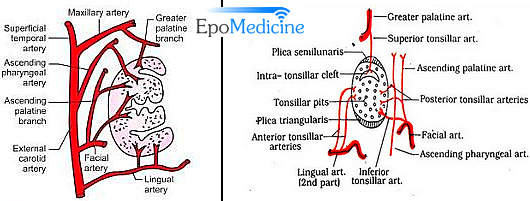
- Anterior tonsillar artery (1): from dorsal lingual branches of lingual artery
- Posterior tonsillar artery (2): from ascending palatine branch of facial, and ascending pharyngeal arteries
- Superior tonsillar artery (1): from greater palatine branch of maxillary artery
- Inferior tonsillar artery (1; main artery): from facial artery
Venous drainage:
- Tonsillar vein → Common facial vein
- Paratonsillar vein → Pharyngeal venous plexus or Common facial vein → Internal Jugular Vein (IJV)
Lymphatic drainage:
Upper deep cervical lymph nodes: Also known as tonsillar lymph nodes
Nerve supply:
- Glossopharyngeal nerve (CN IX)
- Greater and lesser palatine nerve (CN V)
Waldeyer’s ring:
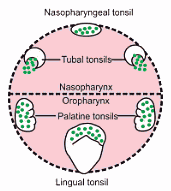 This is a ring of lymphatic tissue at the beginning of food and air passages (in the nasopharynx and oropharynx). The ring is composed of MALT which is characterized by the close approximation of epithelium and lymphatic tissue. The components are:
This is a ring of lymphatic tissue at the beginning of food and air passages (in the nasopharynx and oropharynx). The ring is composed of MALT which is characterized by the close approximation of epithelium and lymphatic tissue. The components are:
- Palatine tonsils (largest) on either side on lateral wall of oropharynx
- Nasopharyngeal tonsil (adenoids) on the posterior wall of nasopharynx
- Tubal tonsils on lateral walls of nasopharynx
- Lingual tonsils on the dorsum of posterior 1/3 of tongue in the floor of oropharynx
Embryology:
- 2nd pharyngeal pouch endoderm: Mucosa and crypts
- Surrounding mesenchyme tissue: Lymphoid tissue
Functions of tonsil:
The activity of this lymphatic organ is especially pronounced during childhood, when immunologic challenges from the environment induce hyperplasia of the palatine tonsils. Following this “active phase” of immune initiation, which lasts until about 8–10 years of age, the lymphatic tonsillar tissue becomes less important as an immune organ, and there is a corresponding decline in the density of lymphocytes in all regions of the tonsils. While the tonsils become less important immunologically with ageing, the tonsillar tissue continues to perform immune functions even at an advanced age, although this should not alter the decision to remove the tonsils if a valid indication for tonsillectomy exists.
Difference between Adenoid and Tonsil:
| Adenoid | Tonsil |
| Ciliated columnar epithelium | Non-keratinizing squamous epithelium |
| No capsule | Hemicapsule |
| Has furrows | Has crypts |
| Peak growth: 6 years | 8 years |
| Growth stops: 12 years | 15 years |
| Disappears: 20 years | Partial regression: 18 years |
Difference between Tonsil and Lymph node:
| Tonsil | Lymph node |
| Subepithelial | Connective tissue |
| Hemicapsule | Fully encapsulated |
| Efferent only | Afferent and Efferent |
| Crypts present | Absent |
| Cortex or medulla absent | Present |
| Growth curve present | absent |
Applied anatomy:
1. Accumulation of pus in in the peritonsillar space in chronic tonsillitis gives rise to peritonsillar abscess or quinsy. It is drained by an incision in the most prominent part of the abscess where softening can be felt.
2. Jugulo-digastric lymph node is often enlarged in tonsillitis.
3. Tonsils prevent infection but when these are infected, acts as septic foci of the body which require surgical removal.
4. Peritonsillar space is the plane of dissection during tonsillectomy.
5. In tonsillectomy, the tonsil is dissected out along with its capsule from its bed.
6. Internal carotid artery, although only 1 inch (2.5cm) behind the tonsil, is never injured in this operation since it lies safely freed from the pharynx by fatty tissue around the carotid sheath.
7. Almost always in surgery, clots are not removed to prevent hemorrhage, but this rule doesn’t apply to tonsils and uterus. After tonsillectomy, blood clots present in the tonsillar fossa are removed. This is done to prevent post-operative hemorrhage because the clots in the tonsillar fossa interfere with the retraction of vessel walls by preventing the contraction of surrounding muscles i.e. the muscles forming boundaries of the tonsillar fossa.
8. Ligature of the tonsillar arteries specially inferior tonsillar artery is important during tonsillectomy.
9. During tonsillectomy, paratonsillar vein may be damaged causing excessive hemorrhage.
10. Referred pain from the tonsils sometimes may radiate into the middle ear due to common nerve supply (CN IX).
11. After tonsillectomy, glossopharyngeal nerve may be affected which causes loss of taste sensation.

Nice collection of info. Contains everything required for MBBS 2nd yr students for this topic.
Fantastic material. Thanks! 😊
I am suffering from CRYPTA MAGNA both sides, any suggestions for me.
Best Regards
Samar
+91 9319003225
U can’t suffer from crypta magna…. Its just the name of the largest crypt in the tonsil. Everyone has that!!! What’s exactly your problem?
What an amazing and informative article..God bless u